VTE Prophylaxis in Surgical Patients

Enoxaparin in VTE Prophylaxis in Cancer Surgery
Landmark trials of enoxaparin in cancer surgery
Enoxacan Study Group (Enoxaparin and cancer)
European, multicenter, double-blind, parallel group study¹

Study Design¹
Treatment Groups¹
- Enoxaparin, administered 40 mg subcutaneously [SC] (either in the lateral abdominal wall or in the thigh) qd with the first dose given 2 hours prior to surgery and continuing for 10±2 days in 555 patients. was compared to
- UFH 5,000 IU SC every 8 hours (q8h) in 560 patients.
Primary Endpoint¹
- The primary endpoint was VTE determined by bilateral ascending venography within 24 hours after the last injection of drug.
- Efficacy was determined in all-treated patients as well as in evaluable patients, who met the protocol entry criteria.
- Of the 1,115 all-treated patients, 631 (56.6%) were evaluable (UFH; n=319, enoxaparin; n=312).
Results: Efficacy¹
The total incidence of DVT and PE in the evaluable patients
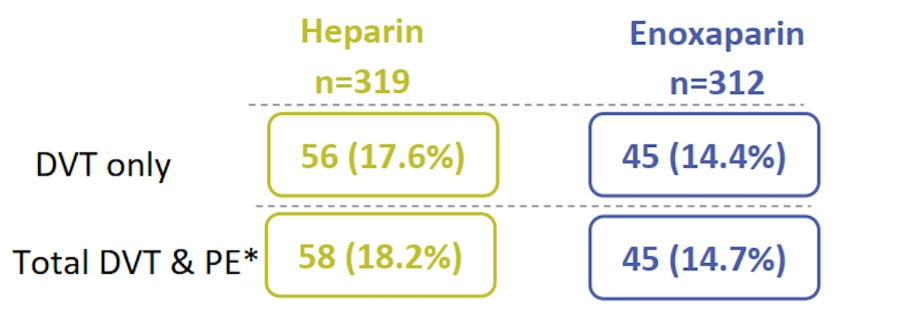
* In the evaluable-patients, PE was diagnosed in 2 patients in the UFHtreated group versus none in the enoxaparin treated group
Results: Safety¹
- Two deaths occurred in the enoxaparin-treated group due to thromboembolic origin.
- Major bleeding* was seen in 4.1% (23/555) of the enoxaparin-treated patients and in 2.9% (16/560) of the UFH-treated patients.
* Defined as hemorrhage caused by a significant clinical event or a drop in hemoglobin of ≥2.0 g/dL or a transfusion of ≥2 units of packed red cells.

The authors concluded that enoxaparin 40 mg SC qd was as effective and safe as UFH SC q8h in preventing thromboembolism after surgery for abdominal and pelvic malignancy.¹
Enoxacan II Study
Multicenter, prospective, double-blind, placebo-controlled, parallel-group, randomized study²
Objective²
Evaluate the efficacy and safety of prolonged thromboprophylaxis with enoxaparin for prevention of VTE after elective, curative surgery for abdominal malignancy. A standard thromboprophylaxis regimen of enoxaparin, given for 1 week, was compared with a prolonged regimen of enoxaparin given for 4 weeks.
Study Design²
In the open phase of the study
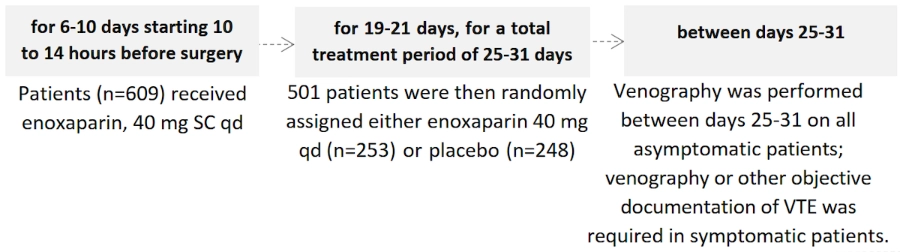
Primary efficacy endpoint: The incidence of VTE between days 25-31.2
Secondary efficacy endpoint: The incidence of death from thromboembolic disease before 3 months.2
Primary safety endpoint: The incidence of hemorrhage during the double-blind treatment period. 2
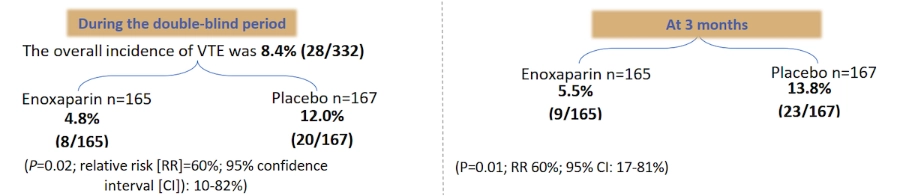
Results: Efficacy²
- Of the 613 patients recruited, 501 underwent randomization and 332 (165 and 167 for enoxaparin and placebo, respectively) had evaluable venograms.
- The mean duration of treatment was 19.3 days in the enoxaparin arm and 19.5 days in the placebo arm.
- Gastrointestinal surgery followed by genitourinary tract, female reproductive organs, palliative, and other surgeries were the most common procedures.
Results: Safety²
- There were no significant differences in major or minor hemorrhage or other serious adverse events (AEs) during the double-blind period or during the 2-month follow-up period.
- None of the showed thrombocytopenia during either period and there were no deaths during the double-blind period.
- During the 2-month follow-up period, 6 patients (3.6%) died in the placebo group and 3 (1.8%) died in the enoxaparin group.
The authors concluded that prophylaxis with enoxaparin for 4 weeks following abdominal or pelvic cancer surgery was safe and significantly reduced the incidence of venographically demonstrated thrombosis compared with enoxaparin prophylaxis for 1 week.²
Enoxacan II Follow-up Study³
Objective³
compared long term, all-cause mortality in the enoxaparin group versus the placebo
Primary Efficacy Endpoint³
Survival at 1 year was the primary efficacy endpoint, however every site had collected survival data beyond 1 year (up to 44 months) and therefore a post hoc analysis utilizing all available data was conducted.
Study Design³
A cox regression model was used to measure prognostic factors, which for the primary analysis, were defined as whether surgery was palliative or curative, and treatment assignment.
Population³
Both treatment groups had similar baseline characteristics, including disease site and risk factors.
Results³
At 1 year there were 243 enoxaparin-treated patients (96%) and 229 placebo-treated patients (92%) with available follow-up data group.
1-year survival rate:3 90.2% for the enoxaparin group and 91.9% for the placebo groups
Palliative surgery:3 The percentage of patients that underwent palliative surgery was significantly greater in the enoxaparin group compared with the placebo group (10.3% vs. 4.0%; P <0.05).
Curative surgery:3 Curative surgery was a more significant prognostic factor compared with palliative surgery (hazard ratio [HR]=0.099; P=0.0001).
- Neither the interaction between type of surgery and treatment nor the treatment effect were significant.3
- At the longest follow-up time periods (43.3 months for the enoxaparin group and 43.5 months for the placebo group), increased survival was greater in the enoxaparin group (HR=0.47, P=0.078). 3
- The mortality rate was significantly greater (P <0.0001) in patients who underwent palliative surgery compared with curative surgery. 3
- After adjustment for the type of surgery, there was a tendency towards decreased mortality among patients undergoing palliative surgery in the enoxaparin group (HR=0.598; P=0.3565) which increased after the 1-year follow-up period (HR=0.469; P=0.078). 3
The authors concluded that further studies are needed to evaluate the effect of prolonged prophylaxis with enoxaparin in cancer patients undergoing palliative surgery on long-term survival. 3
VTE, Venous thromboembolism; DVT, Deep vein thrombosis; PE, Pulmonary embolism; qd, once a day; q8h, every 8 hours; UFH, Unfractionated heparin; IU, International unit
- British Journal of Surgery, 1997. Efficacy and safety of enoxaparin versus unfractionated heparin for prevention of deep vein thrombosis in elective cancer surgery: A double-blind randomized multicentre trial with venographic assessment. 84(8), pp.1099-1103.
- Bergqvist, D., Agnelli, G., Cohen, A., Eldor, A., Nilsson, P., Le Moigne-Amrani, A. and Dietrich-Neto, F., 2002. Duration of Prophylaxis against Venous Thromboembolism with Enoxaparin after Surgery for Cancer. New England Journal of Medicine, 346(13), pp.975-980.
- Bergqvist, D., Agnelli, G., Cohen, A., Nilsson, P., Moigne-Amrani, A. and Dietrich-Neto, F., 2006. Prolonged prophylaxis against venous thromboembolism with enoxaparin in patients undergoing cancer surgery: long-term survival analysis. Phlebology: The Journal of Venous Disease, 21(4), pp.195-198.

Impact of anemia on long-term clinical outcomes in venous thromboembolism: Findings from Garfield-VTE registry

Safety profile of preoperative administration of low-molecular-weight heparin for Lung Cancer population
This randomized clinical trial demonstrated that preoperative administration of low-molecular-weight-heparin (LMWH) is safe and feasible for lung cancer patients preparing to receive minimally invasive surgery.