Real World Evidence Impact of universal immunization with Nirsevimab

Summary of Effectiveness & Reduction of RSV-Hospitalization Estimates
| LEGEND |
|---|
| Effectiveness (Case Controlled) RSV-Hospitalization Reduction (compared to previous years) |

Countries that have implemented nirsevimab
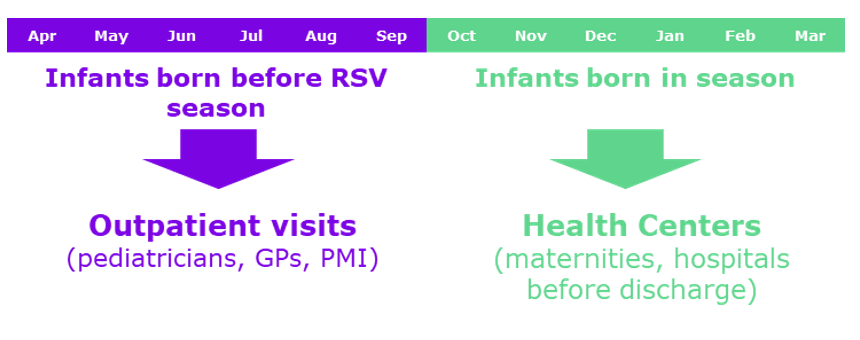
Implementation of nirsevimab to reach infants in US
When?
- From October through end of March in most continental states*
- Within first week of life for infants born during the RSV season, or shortly before or promptly after discharge for infants with prolonged birth hospitalizations
For Whom?
Infants <8 months entering their first RSV season
- Nirsevimab is not needed for most infants aged <8 months whose mother received RSVpreF vaccine ≥14 days before birth2
Infants and children aged 8–19 months who are at increased risk for severe RSV disease and entering their second RSV season**
Who Pays?
- Vaccines for Children (VFC)
- Private insurance
Where?
- Birthing facilities
- Pediatric provider offices
How?
- Standing order or prescription
- Administration by a licensed HCP
*Can adjust administration schedules based on local epidemiology (e.g. Alaska and Hawaii)
**Children with chronic lung disease of prematurity who required medical support (chronic corticosteroid therapy, diuretic therapy, or supplemental oxygen) any time during the 6-month period before the start of the second RSV season, Children with severe immunocompromise, Children with cystic fibrosis who have either 1) manifestations of severe lung disease (previous hospitalization for pulmonary exacerbation in the first year of life or abnormalities on chest imaging that persist when stable) or 2) weight-for-length <10th percentile, American Indian or Alaska Native children
- Jones JM et al, Morb Mortal Wkly Rep 2023;72:920–925. 2. Flemin-Dutra KE et al, Morb Mortal Wkly Rep 2023;72:1115-1122.
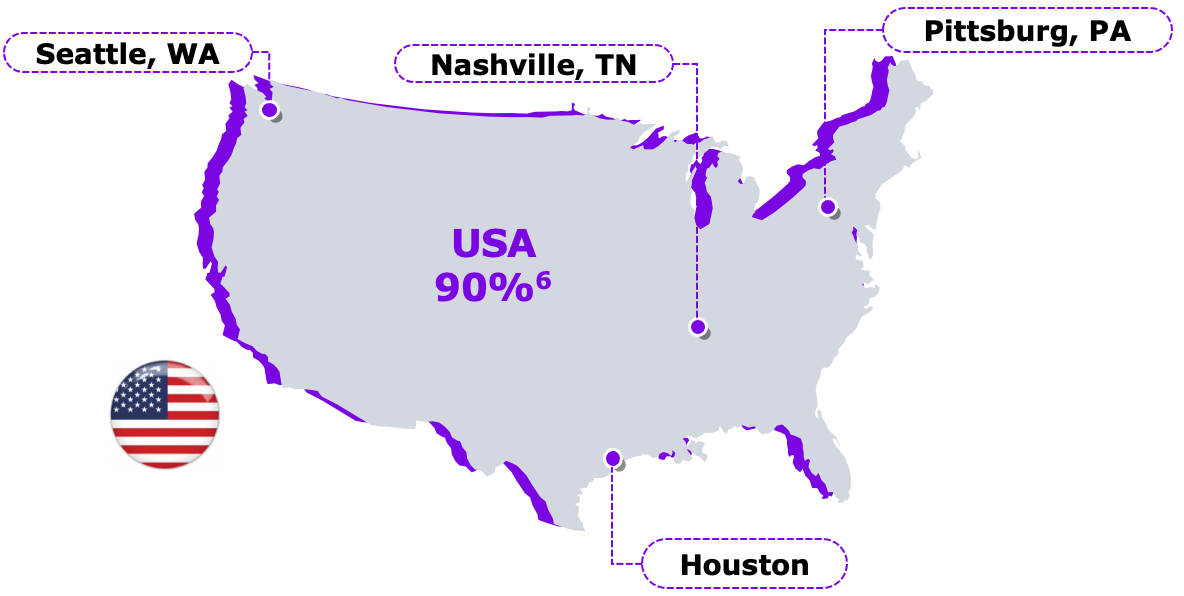
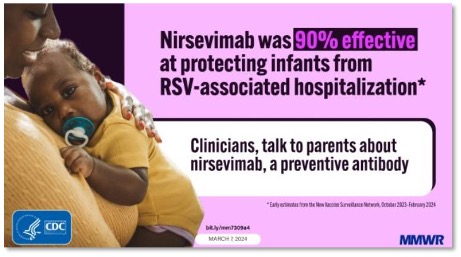
Early Estimate of Nirsevimab Effectiveness for Prevention of RSV-Associated Hospitalization (Oct 2023– Feb 2024)
Study Methodology:
- Test-negative, case-control study from the New Vaccine Surveillance Network of 699 infants enrolled at 4 sites.
- Nirsevimab recipients had a median interval of 45 days (IQR = 19–76) between receipt of nirsevimab to ARI symptom onset.
- Effectiveness was estimated using a regression model that controlled for age, month of illness, site, and and presence of one or more high-risk medical conditions for severe RSV disease.
Implications for Public Health Practice as per CDC:
“Receipt of a single dose of nirsevimab was highly effective against RSV-associated hospitalization in infants entering their first RSV season.”
- Moline HL, et al. MMWR Morb Mortal Wkly Rep 2024;73:209–214.
Nirsevimab Receipt and Intent for Infants Survey - US
Monthly Nirsevimab Receipt and Intent Among Females Aged 18-49 Years, United States
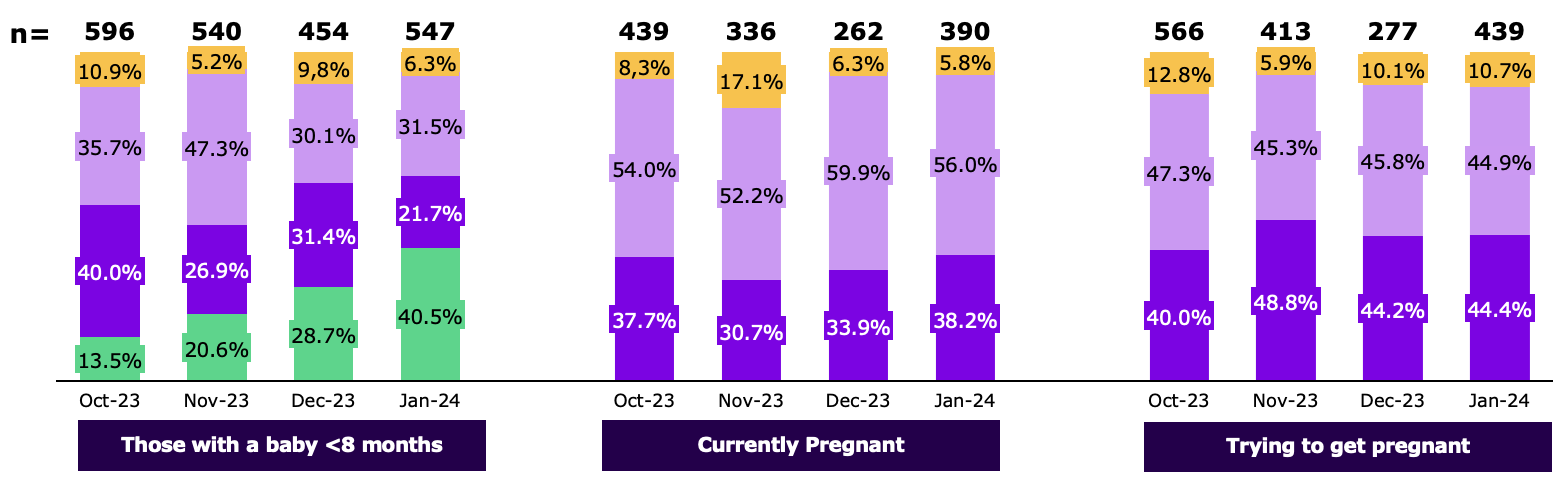
 Probably or definetly will not get nirsevimab for baby
Probably or definetly will not get nirsevimab for baby
 Probably or definetly will get nirsevimab for baby or unsure
Probably or definetly will get nirsevimab for baby or unsure
 Definetly will get nirsevimab for baby
Definetly will get nirsevimab for baby
 Baby got nirsevimab
Baby got nirsevimab
- NIS Adult COVID Module (NIS-ACM) Hard Copy Questionnair https://www.cdc.gov/vaccines/imz-managers/nis/downloads/NIS-ACM-Questionnaire-Q1-2024-508.pdf Published Q1 2024(Accessed 05 Feb 2024)
- Nirsevimab Receipt and Intent for Infants, United States https://www.cdc.gov/vaccines/imz-managers/coverage/rsvvaxview/nirsevimab-coverage.html (Published January 10/2024 Accessed 08 Mar 2024)
Implementation of nirsevimab to reach infants in France
From When?
- From Sep 15, 2023-End of Season
For Whom?
- All infants born after the February 6th to protect during their 1st RSV season
How?
- Mandatory medical prescription needed (doctor or midwife)
- Administration by a doctor, a licensed nurse or a midwife
Where?
- In health care centers
- Outpatients (available in pharmacies)
GP: general practice
PMI: protection maternelle infantile
Parents acceptance were higher than previously estimated by French authorities
- DGS-URGENT N°2023_14 https://sante.gouv.fr/IMG/pdf/dgs-urgent_2023-14_-_traitement_preventif_vrs.pdf (Published: 24/08/2023 Accessed 12 of March 2024)
Bronchiolitis Decline Continues;
Nirsevimab’s Impact Uncertain in France without specific data
Compared to previous seasons, and at this stage of the epidemic, bronchiolitis-related activities are:
<3 months old:
lower than those of the seasons before the emergence of Covid-19;
close to or slightly lower than those in the 2021-2022 season lower than those in the 2022-2023 season.
3-11 months:
generally close to the activities observed during the 2021-2022 and 2022-2023 seasons (ER visits and hospitalization) lower or comparable to those in the seasons before the emergence of Covid-19, except for hospitalization rates after ER remain within the values).
Differences in terms of the impact of the bronchiolitis epidemic observed between infants <3 months of age and infants 3 - 11 months cannot be certainly directly linked to the deployment of nirsevimab treatment on national territory, even if it is the youngest infants who have preferentially been able to benefit from maternity treatment.
The syndromic data of the Oscour network do not make it possible to identify infants who have been able to benefit from this preventive treatment, or to identify infants with RSV bronchiolitis.
- https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/grippe/documents/bulletin-national/infections-respiratoires-aigues-grippe-bronchiolite-covid-19-.-bulletin-du-31-janvier-2024 (Published 31 January 2024, Accessed in March 14th 2024)
- https://www.santepubliquefrance.fr/media/files/01-maladies-et-traumatismes/maladies-et-infections-respiratoires/infections-respiratoires-aigues/annexe_bronchio_france_1-12_mois_20240131 (Published 31 January 2024, Accessed in March 14th 2024)
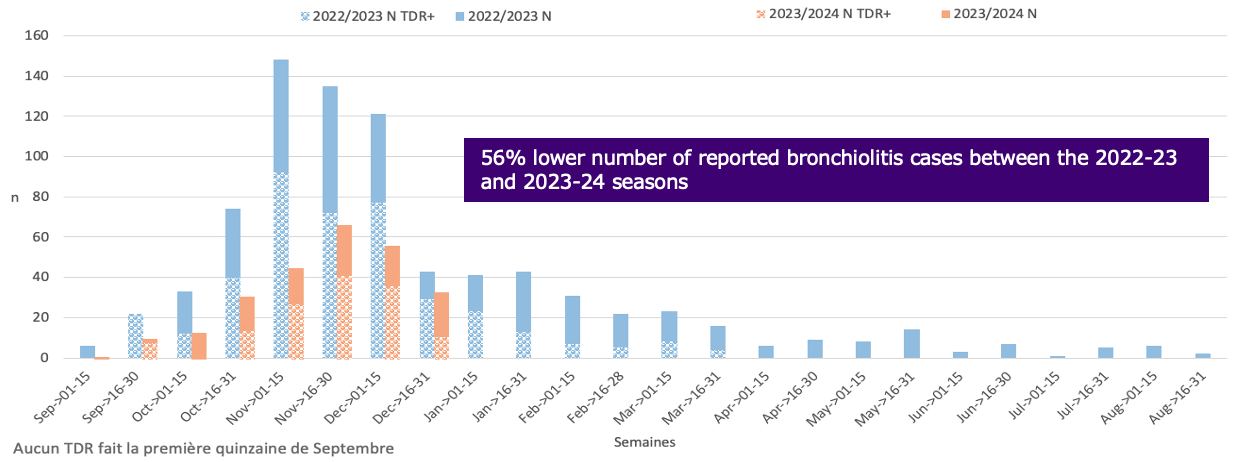
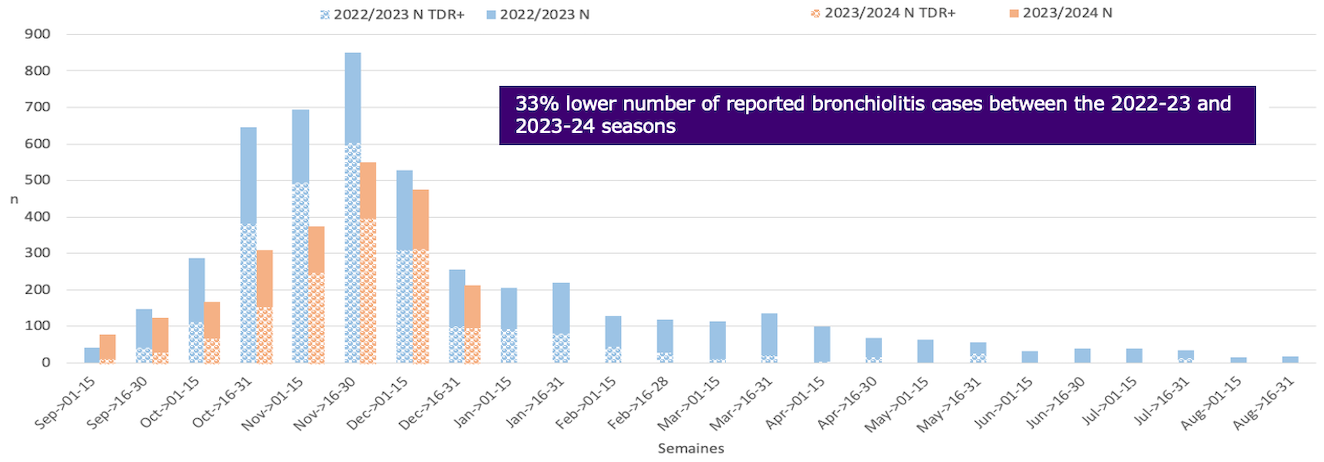
Comparing bronchiolitis episodes before and after nirsevimab implementation (Infovac Sentinel)
RSV cases reduction observed in the target group of immunization
Over 70% of infants born since mid-Sep 2023 til 31st December have been immunized with nirsevimab
Data as of 31st of December, 2023. IRAP Network (ACTIV/AFPA)
- https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/grippe/documents/bulletin-national/infections-respiratoires-aigues-grippe-bronchiolite-covid-19-.-bulletin-du-31-janvier-2024 (Published 31 January 2024, Accessed in March 14th 2024)
- https://www.santepubliquefrance.fr/media/files/01-maladies-et-traumatismes/maladies-et-infections-respiratoires/infections-respiratoires-aigues/annexe_bronchio_france_1-12_mois_20240131 (Published 31 January 2024, Accessed in March 14th 2024)
Impact of Nirsevimab in bronchiolitis episodes (Infovac Sentinel)
Jan 2024
“The key change is the efficacy of Nirsevimab (confirmed above 80%) in France, with the very significant decrease in the number of cases before the age of 3 months.”
- Infovac France Newsletter Newsletter N°10 - November 2023 | Infovac France (Published 28th of November 2023, accessed 12 of March 2024)
Implementation of nirsevimab to reach infants in Spain
From When?
- From Sep 2023 (autonomous communities rollout dates can vary)
How?
- Standing order or prescription
- Administered by a doctor or licensed nurse
For Whom?
- Infants under 6 months at the start of RSV season (born from 1Apr2023 to 31Mar2024
- Children up to 24 months with certain conditions)*
- Minor variations can be observed in the regions‡
Where?
- Galicia: Initial rollout in hospitals (3 week rapid campaign) followed by catch up administration in primary care.
- Madrid: all in hospitals
- Rest of Spain: born in season in the hospital and catch-up in primary care
Who Pays?
- Public funding for families and health care centers
*- Preterm infants below 35 weeks gestational age. - Infants with bronchopulmonary dysplasia64. - Infants with congenital heart disease with significant hemodynamic impairment (those being treated for congestive heart failure, those with moderate or severe pulmonary hypertension, and children with cyanotic heart disease). - Infants with severe immunosuppression due to oncohaematological processes, primary immunodeficiencies (especially combined immunodeficiencies and congenital agammaglobulinemia). ‡ Castilla y Leon:Under 7 months: From 1st March 2023;Pais Vasco: Under 3 months: From 1st July 2023,Navarra: In season
- Martinon-Torres et al. Euro Surveill 2023, 28:pii=2300606
- Calendario de inmunizaciones. https://vacunasaep.org/profesionales/calendario-de-inmunizaciones-aep-2024 published January 1st 2024, accessed 12 March 2024 43. Recomendaciones de utilización de nirsevimab https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/comoTrabajamos/docs/Nirsevimab.pdf, published July 2023,accessed 12 of March 2024
The deployment of Nirsevimab capitalized on existent immunization frameworks, facilitating its assimilation into routine vaccine administration practices.
1. Burden of Disease
Evidence of RSV burden in all infants and surveillance generated1,5
2. Regulatory & scientific societies endorsement
EMA approved2 and pediatric society (AEP)3recommended nirsevimab for prevention of RSV in all infants during their first RSV season
3. NIP inclusion
As for any vaccine-like product, a NITAG4 multidisciplinary working group evaluated and recommended nirsevimab based on :
- Scientific
- Epidemiological
- Ethical
- Political
- Economical
AEP: Spanish Academy of Pediatrics, EMA: European Medicines Agency , NIP: National Immunization Program
- Wildenbeest JG et al. Lancet Respir Med. 2023 Apr;11(4):341-353. doi: 10.1016/S2213-2600(22)00414-3. Epub 2022 Nov 10.
- EMA New medicine to protect babies and infants from respiratory syncytial virus (RSV) infection https://www.ema.europa.eu/en/news/new-medicine-protect-babies-and-infants-respiratory-syncytial-virus-rsv-infection published 16 September 2022, accesse 12 of March 2024
- Calendario de inmunizaciones. https://vacunasaep.org/profesionales/calendario-de-inmunizaciones-aep-2024 published January 1st 2024, accessed 12 March 2024
- Recomendaciones de utilización de nirsevimab https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/comoTrabajamos/docs/Nirsevimab.pdf, published July 2023. accessed 12 of March 2024
- Martinón-Torres, Fet al. BMC Infect Dis 23, 385 (2023).
Successful implementation demonstrated by high coverage
Galicia, Spain is conducting an impact study on nirsevimab and RSV
| Group | Number of Immunized (as of Feb 25th, 2024) | % Coverage Rate |
|---|---|---|
| At birth | 5,638 | 92.7% |
| Catch-up | 6,234 | 85.3% |
| Increased Risk | 349 | 100% |
| Total | 12,221 |
- Martinon-Torres et al. ESWI Respiratory Virus Summit 2024 | ESWI 5th of March 2024 Brussels & online
Impact of Nirsevimab implementation in Galicia
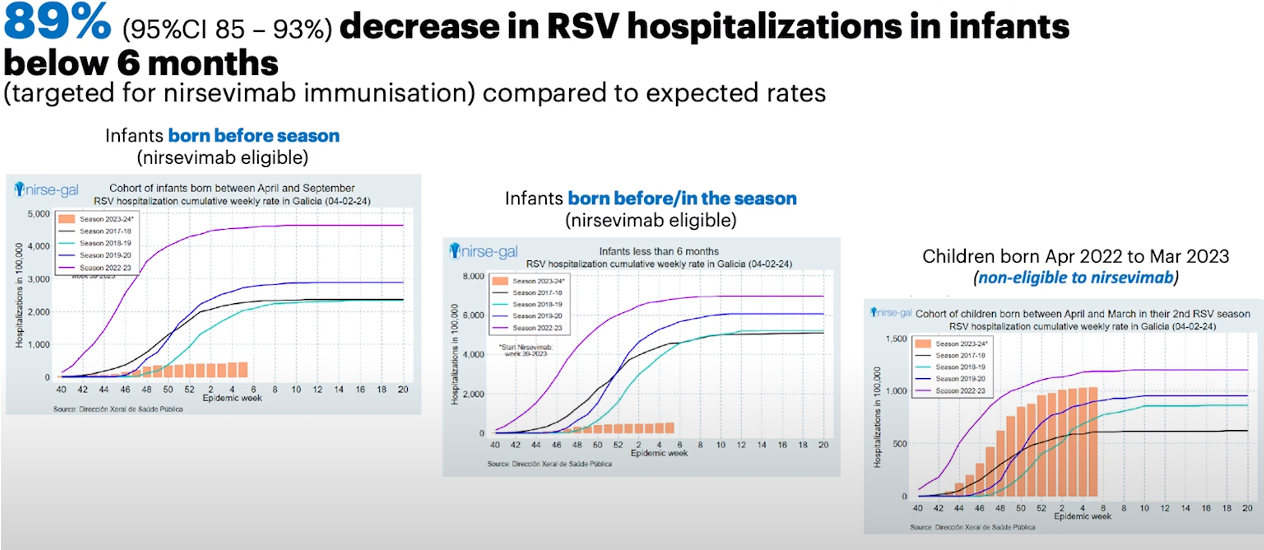
- Results of implementation of Nirsevimab in Galicia Nirsegal.com published February 2024 accessed march 2024
- Martinon-Torres et al. ESWI Respiratory Virus Summit 2024 | ESWI 5th of March 2024 Brussels & online
Cumulative cases in other age groups not lower than previous seasons in children 1 to 4 years old and older than 60 years, not targeted for nirsevimab immunization
~%30
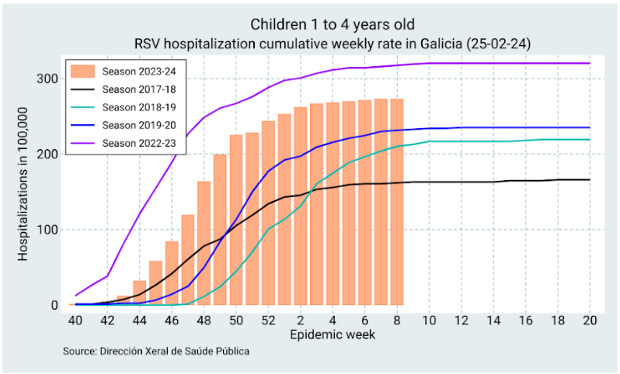
~%330
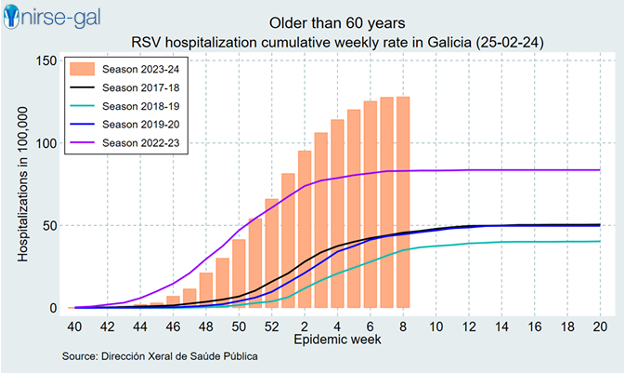
Higher cumulative case number than median of previous seasons
Weekly RSV hospitalization rate in Galicia by season, week 8 2024
- Results of implementation of Nirsevimab in Galicia Nirsegal.com published February 2024 accessed March 2024 2. Martinon-Torres et al. ESWI Respiratory Virus Summit 2024 | ESWI 5th of March 2024 Brussels & online
Effectiveness of Nirsevimab Against RSV-Related Outcomes in Hospital and Primary Care Settings
A Retrospective Cohort Study in Infants in Catalonia (Spain)
| Outcome | N | Rate per 100,000 person days | N | Rate per 100,00 person days | Adjusted hazard ratio (95% CI) | Effectiveness |
|---|---|---|---|---|---|---|
| ICU admission | 17 | 2.13 | 8 | 0.33 | 0.099 (0.041 to 0.237) | 90.1% (76.3% to 95.9%) |
| Hospital admission | 76 | 9.55 | 52 | 2.16 | 0.124 (0.086 to 0.179) | 87.6% (82.1% to 91.4%) |
| Viral pneumonia | 14 | 2.06 | 42 | 1.79 | 0.393 (0.203 to 0.758) | 60.7% (24.2% to 79.7%) |
| Hospital emergency visits | 354 | 45.1 | 604 | 25.5 | 0.446 (0.385 to 0.516) | 55.4% (48.4% to 61.5%) |
| Primary care attended bronchiolitis | 617 | 93.9 | 1,560 | 69.7 | 0.519 (0.467 to 0.576) | 48.1% (42.4% to 53.3%) |
| RSV infection | 31 | 4.57 | 71 | 3.04 | 0.311 (0.200 to 0.483) | 68.9% (51.7% to 80.0%) |
Findings: Among 26,525 infants, a dose of nirsevimab led to an adjusted HR for hospital admission due to RSV bronchiolitis of 0·124 (0·086 to 0·179) and an adjusted HR for ICU admission of 0·099 (0·041 to 0·237). Additionally, the adjusted HR observed for emergency visits was 0·446 (95% CI: 0·385 to 0·516), 0·393 (95% CI: 0·203 to 0·758) for viral pneumonia, 0·519 (95% CI: 0·467 to 0·576) for bronchiolitis attended in primary care, and 0·311 (95% CI: 0·200 to 0·483) for RSV infection. Sensitivity and negative control outcome analyses supported these findings.
- Coma E. et al, Preprints with the Lancet, available at SSRN: https://ssrn.com/abstract=4749763
Implementation of nirsevimab to reach infants in Luxembourg
From When?
- From Oct 1st 2023
Who Pays?
- Public Funding
How & Where?
- Born outside season: pediatric provider's office
- Born in season: maternity hospital (Before discharge)
For Whom?
- All neonates born between 1 October 2023 and 30 March 2024
- Infants born from 1 January until 30 September 2023 (i.e. catch-up immunization)
- Children under the age of 2 years with risk factors for severe respiratory infection
Recommandations du Conseil supérieur des maladies infectieuses concernant l’immunisation passive contre le RSV par des nouveaux anticorps CONSEIL SUPERIEUR D’HYGIENE (public.lu) published July 2023; accessed 14th of March 2024
Luxembourg
- The length of hospital stay was significantly reduced from a mean of 5.1 days (SD: 5.4) in 2022 compared to 3.2 days (SD: 2.5) in 2023 (p < 0.001).
- Infants < 6 months old (5.6 days in 2022 vs 3.4 days in 2023, p < 0.001)
- 78.5% (22/28) of infants up to 6 months of age needing oxygen supplementation were not immunised.
- 69.2% (9/13) received Nasal high flow therapy were not immunized.
- 66.6% (6/9) admitted to PICU were not immunized.
The majority of severe RSV LRTI cases were on non-immunized infants
- Coverage in Maternity wards October to mid-December 2023 was estimated at 84% (from 66% to 94%).
- A decrease of 69% RSV lab-confirmed hospitalizations among infants under 6 months old.
- With a 38% decrease in children under 5 years of age 65.3% of infants under 6 months were not immunized.
Ernst C et al. Euro Surveill. 2024;29(4):pii=2400033.


