The Bright Study

The first head-to-head RCT designed to compare the efficacy and safety of Gla-300 with IDeg-100 in participants with T2DM.
Background

However, direct clinical comparisons between these two-2nd generation basal insulin analogues are not available.
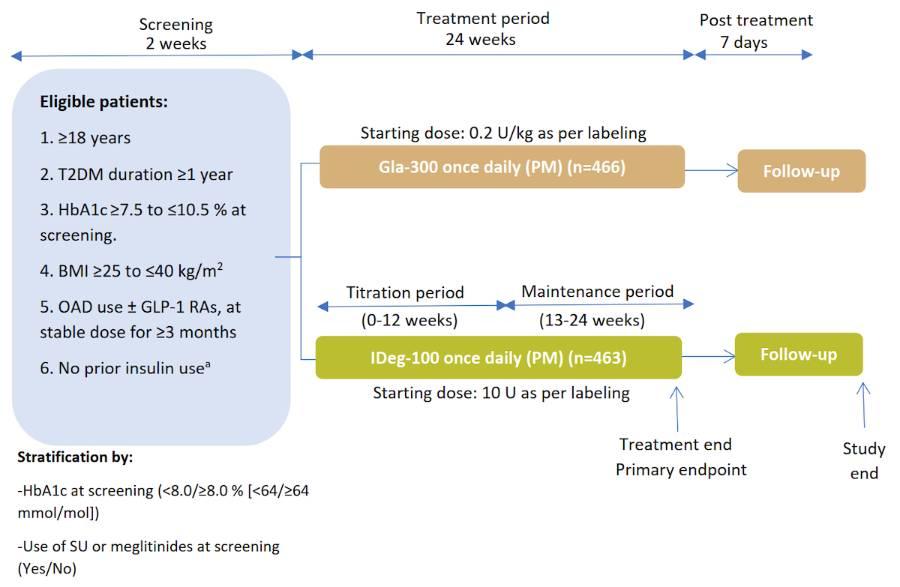
Study Design⁵
Multicentre, open-label, 1:1 randomised, active-controlled, 2-arm parallel-group, non-inferiority study in adult participants with uncontrolled T2DM
%20(1).jpg)
Gla-300 and IDeg-100 were self-administered once daily between 18:00–20:00 h5
Titrated weekly to target fasting SMPG of 4.4–5.6 mmol/L (80–100 mg/dL)
without hypoglycaemia5
Titration performed with aim of target achievement within 8–12 weeks post
randomisation (titration period)5
ᵃDoses titrated at least weekly
aWith the exception of a maximum of 8 consecutive days or 15 days total prior insulin use
Pre-Defined Endpoints⁵
Primary efficacy endpoint:
Change in HbA1c from baseline to week 24
- Analysed using a MMRM approach, adjusted for covariates including baseline HbA1c
Secondary efficacy endpoints:
-
Change in HbA1c and fasting SMPG from baseline to week 12
-
Change in FPG, fasting SMPG and 8-point SMPG profiles from baseline to week 24
-
Variability of 8-point SMPG profiles
Safety endpoints:
-
Incidence and annualised rates of confirmed hypoglycaemia (≤3.9 and <3.0 mmol/L) over the full 24-week period, and during weeks 0–12 (titration period) and weeks 13–24 (maintenance period)
-
TEAEs
Results
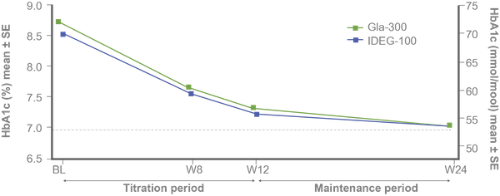
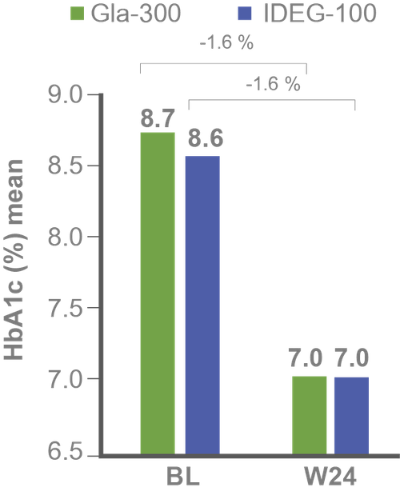
Primary efficacy endpoints:
Non-inferiority of Gla-300 vs IDeg-100 in HbA1c reduction at study end⁵
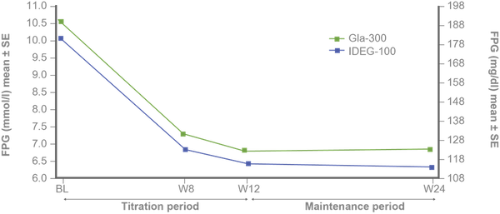
Secondary efficacy endpoints:
FPG and fasting SMPG reduction with Gla-300 vs IDeg-100 from baseline to study end⁵
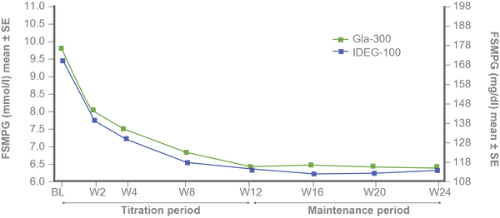
Similar 8-point SMPG and variability profiles at baseline and study end⁵
Similar variability of 24-h SMPG and fasting SMPG at baseline and week 24 with both treatments.⁵

|
Mean CV, % |
Gla-300 |
IDeg-100 |
|
24-h SMPG |
|
|
|
Baseline |
22.5 |
23.4 |
|
Week 24 |
27.6 |
28.0 |
|
LS mean change |
3.7 |
4.0 |
|
Fasting SMPG |
|
|
|
Baseline |
13.8 |
14.6 |
|
Week 24 |
16.5 |
17.0 |
|
LS mean change |
1.5 |
2.0 |
Safety endpoints:
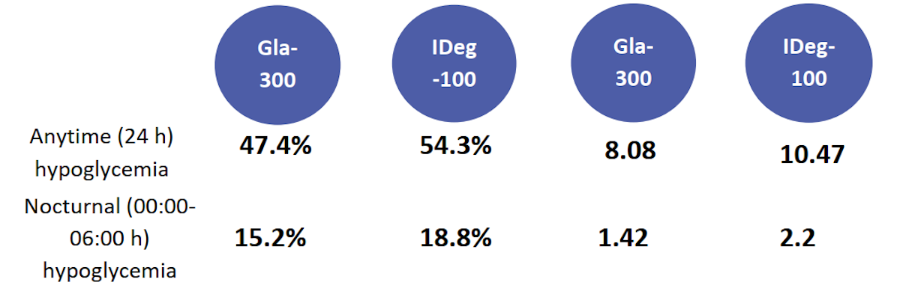
Incidence (%) and events per patient-year of confirmed (≤3.9 mmol/l) during titration period⁵
Treatment-emergent adverse events⁵
-
No specific safety concerns were reported
-
There was one death in the Gla-300 group (adenocarcinoma of the colon)
-
Only one episode of severe hypoglycemia occurred during the entire study.
Confirmed hypoglycaemia included documented symptomatic or asymptomatic hypoglycaemia (≤70 mg/dL or <54 mg/dL), and severe events if any; only 1 participant experienced severe hypoglycaemia (1 event), in the Gla-300 group, due to a skipped evening meal and not reducing her insulin dose after a non-severe event 2 days earlier. All p-values presented are nominal. Safety population (Gla-300, n=463; IDeg-100, n=462)⁵
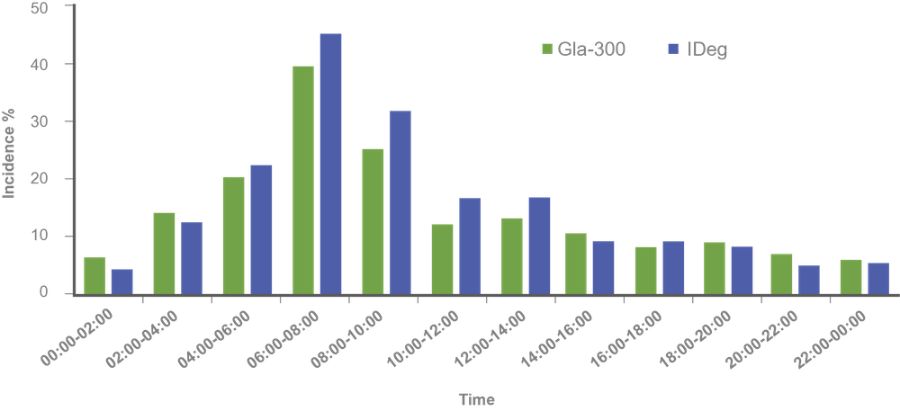
Findings:
Hypoglycemia incidence by time of day⁷
Comparable glycaemic control and hypoglycaemia incidence over 24 weeks, regardless of SU/glinide use at screening⁶
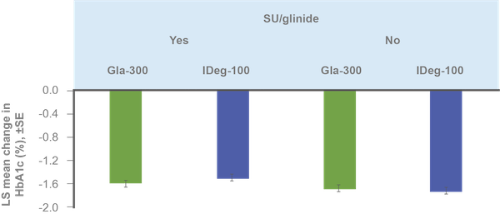
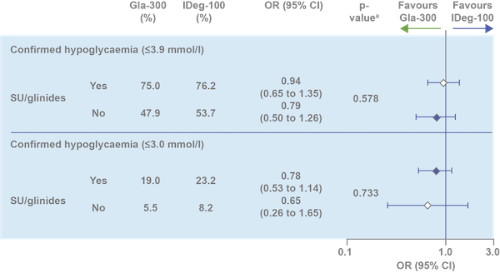
ᵃp value to test heterogeneity of treatment-by-subgroup interaction. HbA1c reduction assessed in ITT population; hypoglycemia incidence assessed in safety population
Clinical Implications
-
Gla-300 and IDeg-100 provide similar glycaemic control accompanied by comparable hypoglycaemia⁵
-
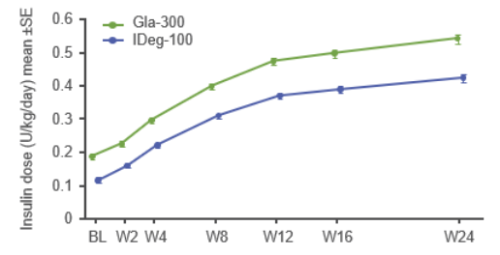
Active and adequate titration can help patients achieve glycaemic goals – dose increases are associated with improved HbA1c levels⁸
-
Early hypoglycaemic events during titration are associated with increased rates of treatment discontinuation, as well as long-term risk of hypoglycaemia⁹,¹⁰
-
Gla-300 may offer an advantage in hypoglycaemia risk reduction vs IDeg-100 during the titration period in insulin-naïve patients with T2DM⁵
Conclusion
-
Bright was the first direct comparison of Gla-300 vs IDeg-100:
-
Similar glycaemic control for HbA1c and fasting SMPG
-
Similar variability in 24-h SMPG and fasting SMPG
-
-
During the full study and maintenance periods, anytime and nocturnal confirmed hypoglycaemia were comparable
-
During the titration period (0–12 weeks), the rate of anytime and nocturnal confirmed hypoglycaemia were lower with Gla-300 vs IDeg-100
Gla-300, insulin glargine 300 U/mL; IDeg-100, insulin degludec 100 U/mL; PK/PD, pharmacokinetic/pharmacodynamic; RCT, randomized clinical trial; T2DM, type 2 diabetes; BMI, body mass index; GLP-1 RA, glucagon-like peptide-1 receptor agonist; OAD, oral antihyperglycemic drug; SMPG, self-monitored plasma glucose; SU, sulfonylureas; FPG, fasting plasma glucose; MMRM, mixed model for repeated measurements; TEAE, treatment-emergent adverse event; BL, baseline; ITT, intention-to-treat; LS, Least square; SE, standard error; W, week; CI, confidence interval; CV, coefficient of variation; SD, Standard deviation.
- Becker, R., Dahmen, R., Bergmann, K., Lehmann, A., Jax, T. and Heise, T., 2015. New Insulin Glargine 300 units {middle dot} mL-1 Provides a More Even Activity Profile and Prolonged Glycemic Control at Steady State Compared With Insulin Glargine 100 units{middle dot}mL-1. Diabetes Care, 38(4), pp.637-643.
- Heise, T., Hermanski, L., Nosek, L., Feldman, A., Rasmussen, S. and Haahr, H., 2012. Insulin degludec: four times lower pharmacodynamic variability than insulin glargine under steady‐state conditions in type 1 diabetes. Diabetes, Obesity and Metabolism, 14(9), pp.859-864.
- Ratner, R., Gough, S., Mathieu, C., Del Prato, S., Bode, B., Mersebach, H., Endahl, L. and Zinman, B., 2013. Hypoglycaemia risk with insulin degludec compared with insulin glargine in type 2 and type 1 diabetes: a pre‐planned meta‐analysis of phase 3 trials. Diabetes, Obesity and Metabolism, 15(2), pp.175-184.
- Ritzel, R., Roussel, R., Bolli, G., Vinet, L., Brulle‐Wohlhueter, C., Glezer, S. and Yki‐Järvinen, H., 2015. Patient‐level meta‐analysis of the EDITION 1, 2 and 3 studies: glycaemic control and hypoglycaemia with new insulin glargine 300 U/ml versus glargine 100 U/ml in people with type 2 diabetes. Diabetes, Obesity and Metabolism, 17(9), pp.859-867.
- Rosenstock, J., Cheng, A., Ritzel, R., Bosnyak, Z., Devisme, C., Cali, A., Sieber, J., Stella, P., Wang, X., Frías, J., Roussel, R. and Bolli, G., 2018. More Similarities Than Differences Testing Insulin Glargine 300 Units/mL Versus Insulin Degludec 100 Units/mL in Insulin-Naive Type 2 Diabetes: The Randomized Head-to-Head BRIGHT Trial. Diabetes Care, 41(10), pp.2147-2154.
- ROUSSEL, R., ROSENSTOCK, J., PETTUS, J., RITZEL, R., CHENG, A., BOSNYAK, Z., DEVISME, C., CALI, A., WANG, X. and BOLLI, G., 2018. Impact of Background Antihyperglycemic Therapy on Insulin Glargine 300 U/mL (Gla-300) vs. Insulin Degludec 100 U/mL (IDeg-100) in Insulin-Naïve People with T2DM from the BRIGHT Randomized Study. Diabetes, 67(Supplement 1), p.1029-P.
- BOLLI, G., CHENG, A., BOSNYAK, Z., CORFEC, E., CALI, A., WANG, X., FRIAS, J., ROUSSEL, R. and ROSENSTOCK, J., 2018. Lower Hypoglycemia Rates with Insulin Glargine 300 U/mL (Gla-300) vs. Insulin Degludec 100 U/mL (IDeg-100) in Insulin-Naïve Adults with T2DM on Oral Antihyperglycemic Therapy ± GLP-1RA—The BRIGHT Randomized Study. Diabetes, 67(Supplement 1), p.1032-P.
- Khunti, K., Caputo, S., Damci, T., Dzida, G., Ji, Q., Kaiser, M., Karnieli, E., Liebl, A., Ligthelm, R., Nazeri, A., Orozco-Beltran, D., Pan, C., Ross, S., Svendsen, A., Vora, J., Yale, J. and Meneghini, L., 2012. The safety and efficacy of adding once-daily insulin detemir to oral hypoglycaemic agents in patients with type 2 diabetes in a clinical practice setting in 10 countries. Diabetes, Obesity and Metabolism, 14(12), pp.1129-1136.
- Dalal, M., Kazemi, M. and Ye, F., 2016. Hypoglycemia in patients with type 2 diabetes newly initiated on basal insulin in the US in a community setting: impact on treatment discontinuation and hospitalization. Current Medical Research and Opinion, 33(2), pp.209-214.
- Mauricio, D., Meneghini, L., Seufert, J., Liao, L., Wang, H., Tong, L., Cali, A., Stella, P., Carita, P. and Khunti, K., 2017. Glycaemic control and hypoglycaemia burden in patients with type 2 diabetes initiating basal insulin in Europe and the USA. Diabetes, Obesity and Metabolism, 19(8), pp.1155-1164.


New technologies in Type 2 Diabetes management and future opportunities to improve clinical outcomes
This session emphasizes that new technology in Diabetes management not only can overcome common barriers in achieving glycemic control in people with T2D but also may facilitate more effective and efficient Diabetes care.
