Fabry Disease in Cardiology Practice: From Red Flags to Diagnosis
Cardiac Manifestations of Fabry Disease
|
• FD is a rare X-linked lysosomal storage disorder caused by α-galactosidase A deficiency, leading to Gb3 accumulation in tissues, including the heart.1
• Cardiac involvement is the leading contributor to reduced QoL and mortality in patients with FD.1
Challenges and unmet needs |
|
Gaps in
|
• Family screening is limited; underlining the need for broader screening initiatives and early intervention.2
• Lack of heart-specific biomarkers for early detection and disease monitoring.3 • Absence of validated prognostic stratification tools to predict cardiac progression and risk.3 |
| • FD remains underdiagnosed due to limited awareness, especially in patients with unexplained LVH.2
• Among cardiologists, diagnosis is often delayed, with initial diagnosis of FD by other specialists, leaving cardiologists for later stage management.4 |
Limited
|
Cardiologists are central to diagnosis, cardiac management, treatment
timing, family screening, and research in FD.4
What cardiologists need to know about FD? |
|
Pathophysiology of cardiac
|
FD mimics common cardiac
|
| • GL-3 accumulates in all cardiac cell types
• Lyso-GL-3 drives cardiomyocyte hypertrophy •Cellular dysfunction occurs early • Progression leads to myocardial fibrosis |
• Typically presents as LVH
• Mimics hypertrophic cardiomyopathy (HCM) |
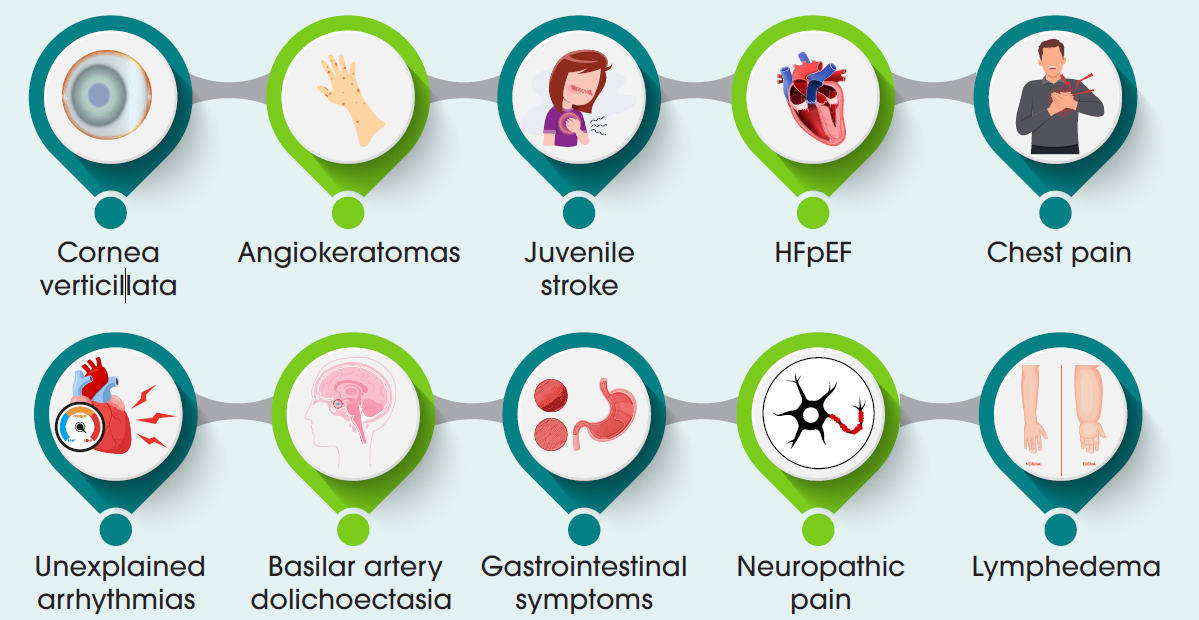
Clinical manifestations1 |
Diagnosing Fabry Disease
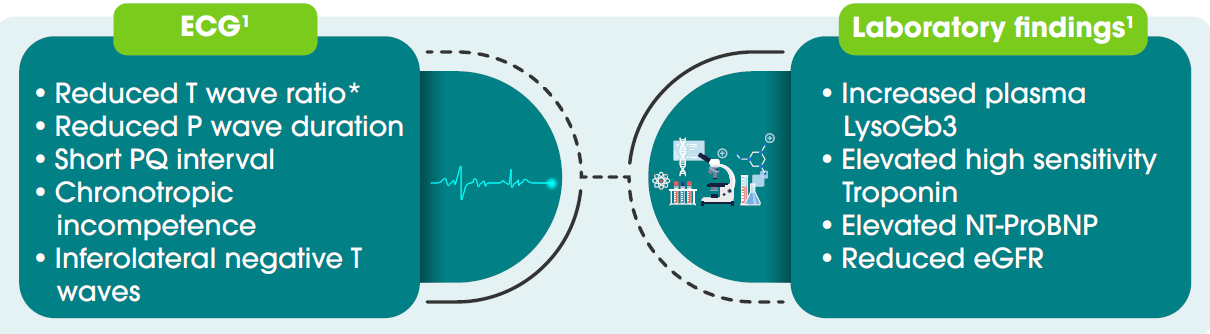
Cardiac imaging1 |

Close collaboration between cardiologists and other specialists is essential for timely diagnosis of FD in patients and to maximize therapy outcomes.1
Abbreviations
FD: Fabry Disease; QoL: Quality of Life; LSD: Lysosomal Storage Disorder; α-Gal A: Alpha-galactosidase A; Gb3 / GL-3: Globotriaosylceramide; Lyso-Gb3 / Lyso-GL-3: Globotriaosylsphingosine; LVH: Left Ventricular Hypertrophy; HCM: Hypertrophic Cardiomyopathy; ECG: Electrocardiography; PQ interval: PR interval; AV block: Atrioventricular block; 2D Echo: Two-dimensional Echocardiography; CMR: Cardiac Magnetic Resonance; LGE: La te Gadolinium Enhancement; T1: Native T1 relaxation time; HFpEF: Heart Failure with Preserved Ejection Fraction; ERT: Enzyme Replacement Therapy; CV: Cardiovascular; CVD: Cardiovascular Disease; IV: Intravenous; GLA: Galactosidase Alpha gene
1. Pieroni M, Moon JC, Arbustini E, Barriales-Villa R, Camporeale A, Vujkovac AC, et al. Cardiac
Involvement in Fabry Disease. JACC. 2021 Feb 23;77(7):922–36.
2. Fabry disease cardiomyopathy: A state-of-the-art review - ScienceDirect [Internet]. [cited 2025 Dec 22]. Available from: https://www.sciencedirect.com/science/article/pii/ S0033062025001148?utm_source=chatgpt.com
3. Pieroni M, Zocchi C, Ciabatti M. Cardiac involvement in Fabry disease: Recent advances, unresolved issues, and unmet needs . [cited 2025 Dec 22]; Available from: https://dx.doi.org/ 10.1093/eurheartjsupp/suae104
4. Pieroni M, Namdar M, Olivotto I, Desnick RJ. Anderson–Fabry disease management: role of the cardiologist. [cited 2025 Dec 22]; Available from: https://dx.doi.org/10.1093/eurheartj/ehae148
5. Hagège A, Réant P, Habib G, Damy T, Barone-Rochette G, Soulat G, et al. Fabry disease in
cardiology practice: Literature review and expert point of view. Archives of Cardiovascular
Diseases. 2019 Apr 1;112(4):278–87.