Prevalence Of LOPD In Patients With Undifferentiated Proximal Myopathy And Undiagnosed Muscle Biopsy

Study objective and method
 Examine patients with
Examine patients with
LGMW and/or
hyperCKemia and
undiagnosed muscle
biopsy for LOPD
Inclusion criteria:
Inconclusive LGMW with
undiagnosed muscle
biopsies
Of the 340
evaluated muscle
biopsies,
69 fulfilled the
inclusion criteria
Testing:
DBS+enzyme
activity of GAA
Results
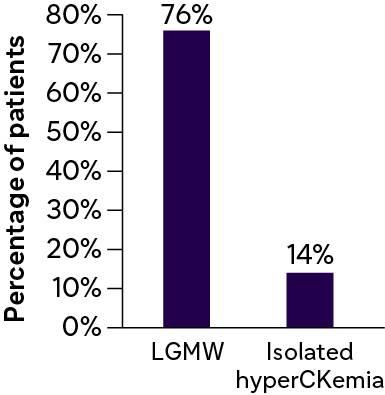
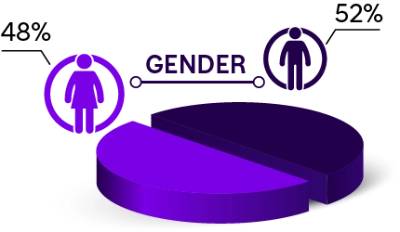
Baseline characteristics of patients with unclassified LGMW
%20(1).2024-03-18-09-01-03.jpg)
.2024-03-18-09-01-03.jpg)

Median age
51 years

Median symptom onset
6 years
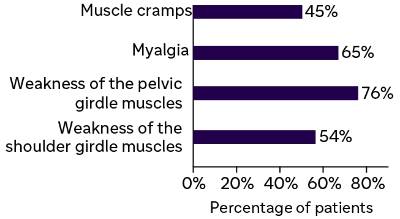
Clinical and laboratory data of patients with unclassified LGMW
Median DBS GAA
activity: 1.18
nmol/punch×21 hours
Reduced GAA activity
was identified through
enzyme kinetic testing
in two patients
Myopathic symptoms
.2024-03-18-09-01-03.jpg)
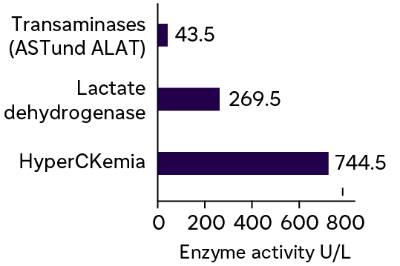
Laboratory results
.2024-03-18-09-01-03.jpg)
Diagnostic yield of LOPD: 2/69 (2.9%)
| Patient 1 |  |
Patient 2 |
| A 22-year–old Caucasian female with the chief complaint of muscular exertion intolerance associated with muscle aches and cramps. |
Patient profile
|
A 29-year–old Caucasian male with atrophies of the shoulder, pelvic girdle, and paravertebral muscles. Predominantly left-sided scapula alata and positive Gower’s sign. |
| Completely unspecific myopathic changes with evidence of small lipid droplets |
Muscle biopsy
|
|
|
No signs of HCM, FVC: <80% |
Other findings
|
No signs of HCM, FVC: 72% |
LOPD not only demonstrates wide variability in the clinical phenotype but also in the histopathological changes in the skeletal muscles.
Conclusion
- Revisiting muscle biopsies is important in neuromuscular disease diagnosis.
- Muscle biopsy can aid in LOPD identification, but glycogen-related vacuolation can be absent.
- An inconclusive muscle biopsy does not rule out Pompe disease.
- DBS evaluation should precede muscle biopsy for all LGMW patients
ALAT: Alanine aminotransferase; AST: Aspartate transaminase; CK: Creatine kinase; DBS: Dried blood spots; FVC: Forced vital capacity; HCM: Hypertrophic cardiomyopathy; LGMW: Limb-girdle myopathic weakness; LOPD: Late-onset Pompe disease.
Golsari A, Nasimzadah A, Thomalla G, et al. Prevalence of adult Pompe disease in patients with proximal myopathic syndrome and undiagnosed muscle biopsy. Neuromuscul Disord. 2018;28(3):257–261.

.png/jcr:content/Asset%201@3x%20(1).png)
Differential Diagnosis Of Late Onset Pompe Disease (LOPD) and Myotonic Dystrophy Type 1 Through Abdominal Ultrasonography
.png/jcr:content/Asset%2010%20(1).png)