Multiple Myeloma: High Risk Cytogenetics

Multiple Myeloma: Cytogenetic abnormalities
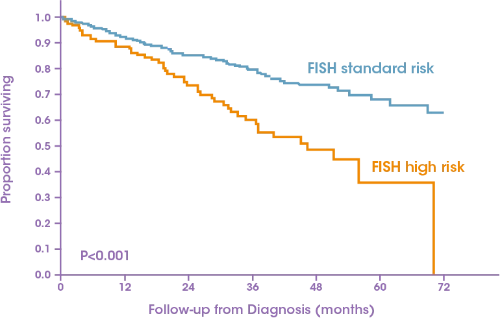
The presence of high-risk cytogenetic features has been well documented as a negative prognostic factor and these patients typically have poorer outcomes compared with standard risk patients1,2
Patients with high-risk cytogenetics are not always captured in clinical trials or real-world studies resulting in subgroup analyses on a relatively small sample
size3–5
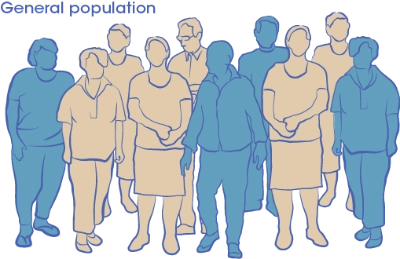.2024-02-06-15-30-12.webp)
Consequently, there is a paucity of data for the targeted treatment of patients with high-risk cytogenetics and randomized trials are needed in these populations5
.2024-02-06-15-31-05.webp)
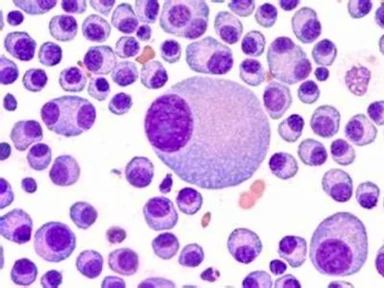
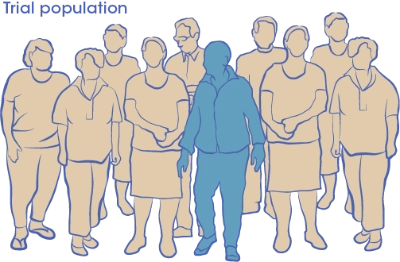
Genomic instability and heterogeneity are hallmarks of multiple myeloma1,6
.2024-02-06-15-32-05.webp)
Multiple myeloma: cytogenetic abnormalities1,6,12

Normal
Trisomies ~50% of cases

Duplications of entire chromosomes
Typically involves chromosomes 3, 5, 7, 9, 11, 15, 19 or 21
Translocations 40–70% of cases

Translocations involving the immunoglobulin heavy-chain gene on chromosome 14
Deletions 7–50% of cases

Loss of chromosomes or sections, resulting in haploinsu ciency
Typically involves chromosomes 1, 6, 8, 13, 11, 14, 16 or 17
Gains ~40% of cases

Duplication of
chromosomes or sections
Frequently a ects
chromosome 1q
Cytogenetic analysis of bone marrow samples by fluorescence in situ hybridization (FISH) is recommended at diagnosis for risk stratification1,13,14
The IMWG use the following cytogenetic abnormalities identified by FISH to define multiple myeloma with poor prognosis:1
t(14;20) 1 % of MM cases

t(14;16) 4% of MM cases*

del(17/17p) 7% of MM cases*

t(4;14) 15% of MM cases*
gain(1q) 40% of MM cases
*Included in the Revised International Staging System for multiple myeloma as high-risk15
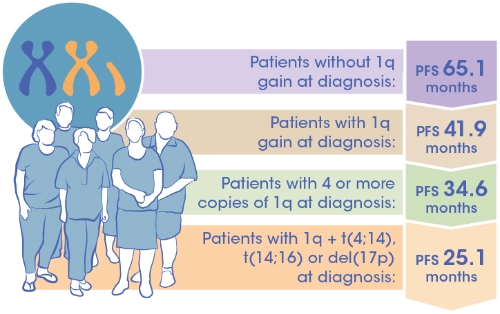
Gain of chromosome 1q is commonly found in patients with MM and frequency increases with disease progression16
Gain 1q is a poor prognostic factor with a negative impact on survival outcomes particularly when there are more than 4 copies present or if it is associated with other high-risk cytogenetic abnormalities
A clear definition of a high-risk diagnosis is needed
Response rates and survival outcomes are lower for patients with genetic abnormalities versus those with standard risk cytogenetics2,17
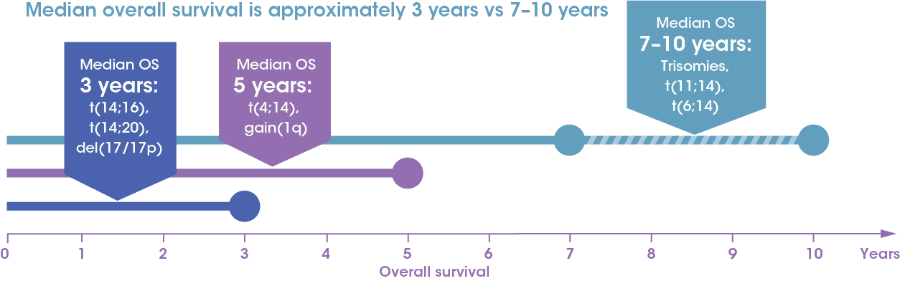
The presence of multiple cytogenetic abnormalities further decreases prognosis compared with individual high-risk abnormalities1,18,19
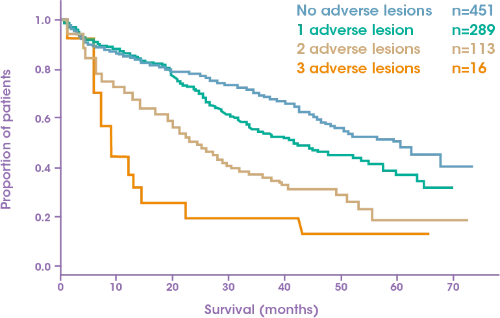
There remains a detrimental gap between high-risk and standard risk cytogenic patients5,7
- Sonneveld P, et al. Blood 2016;127:2955–62;
- Nooka AK, et al. Am Soc Clin Oncol Educ Book 2016;35:e431–41;
- Dimopoulos MA, et al. Cancer Treat Rev 2015;41:827–35;
- Richardson PG, et al. Blood Cancer J 2018;8:109;
- Lancman G, et al. Clin Adv Hematol Oncol 2017;15:870–9;
- Castaneda O and Baz R. Acta Medica Academica 2019;48:57–67;
- Kumar S, et al. Blood 2012;119:2100–5;
- Bianchi G & Ghobrial IM. Curr Cancer Ther Rev 2014;10:70–9;
- Brioli A, et al. Br J Haematol 2014;165:441–54;
- Keats JJ, et al. Blood 2012;120:1067–76;
- Manier S, et al. Nat Rev Clin Oncol 2017;14:100–13;
- Saxe D, et al. Int J Lab Hem 2019;41:5–14;
- NCCN Guidelines Multiple Myeloma V4.2022. Available at: https://www.nccn.org/;
- Moreau P, et al. Ann Oncol 2017;28 (suppl_4):iv52–61;
- Palumbo A, et al. J Clin Oncol 2015;33:2863–9;
- Schmidt TM, et al. Blood Cancer J 2019;9:94;
- Rajkumar SV. Am J Hematol 2016;91:720–34;
- Boyd KD, et al. Leukemia 2012;26:349–55;
- Jian et al. Medicine (Baltimore) 2016;95:e3521
.jpg/jcr:content/jcr_content%20(14).jpg)