RSV Burden in Infants
.jpg/jcr:content/science%20hero%20(9).jpg)
Methods
|
STUDY DESIGN
Compare passive immunization with LA mAb for all infants to the current standard of care using a static decision-analytic model in a cohort of KSA infants experiencing their first RSV season
Subpopulations:
|
PARTICIPANTS & SEASON
Entire KSA infant birth cohort(<12 months of age) during their 1st RSV season
(October – March) |
IMMUNIZATION STRATEGIES
Standard of Care: healthy infants born at least 29w GA, administered monthly to eligible infants during the season
LA mAb (Nirsevimab) Single dose administered to all infants at the beginning of the RSV season or at birth |
ANALYSIS
Static decision-analytic model RSV burden and nirsevimab impact were considered and stratified by:
|

Alharbi, A. S., Alqwaiee, M., Al-Hindi, M. Y., Mosalli, R., Al-Shamrani, A., Alharbi, S., Yousef, A., Al Aidaroos, A., Alahmadi, T., Alshammary, A., Miqdad, A., Said, Y., & Alnemri, A. (2018). Bronchiolitis in children: The Saudi initiative of bronchiolitis diagnosis, management, and prevention (SIBRO). Annals of thoracic medicine, 13(3), 127–143. https://doi.org/10.4103/atm.ATM_60_18
Assumptions
Hospitalizations rates per age groups & subpopulations in local birth cohort in KSA
2021 Saudi birth = 509,139

Highest risk of hospitalizations
Per subpopulation
- Palivizumab eligible: early preterm ≤28 weeks of GA, with CHD or CLDP
- Preterm infants >28 weeks of GA
Per chronological age
- with risk decreasing with increasing age in months
CHD, congenital heart disease; CLDP, chronic lung disease of prematurity; GA, gestational age; mo, month.
Ahmed A, Parveen S, Al-Hassinah SM, Al-Amery SF. An overview of respiratory syncytial virus infections in Saudi Arabia. The Journal of Infection in Developing Countries. 2018;12(11):929-36
- Ministry of Health. Premature Babies 2019 [August 2023]. Available from: https://www.moh.gov.sa/en/awarenessplateform/ChildsHealth/Pages/PrematureBabies.aspx
Results
Disease burden under the current standard of care
 |
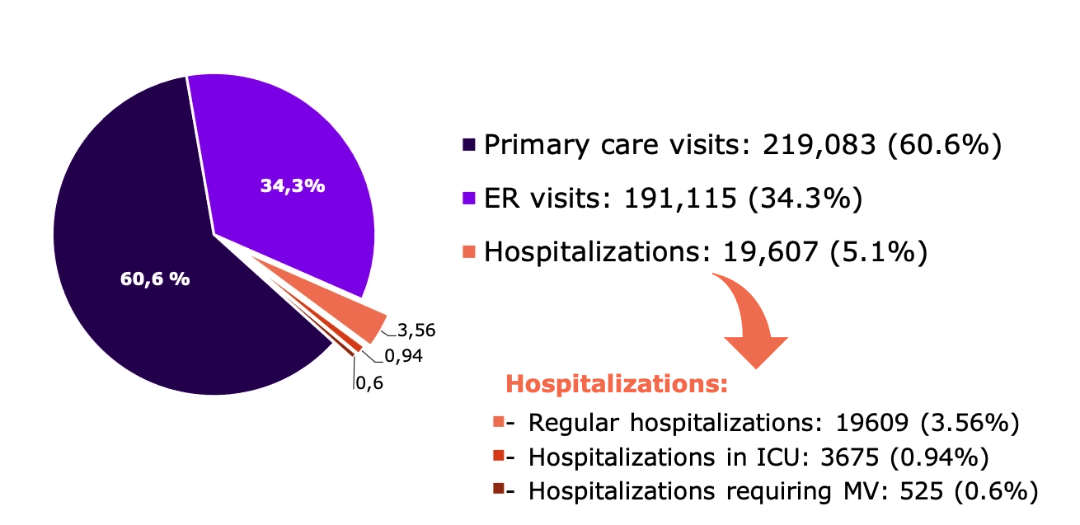
428,264 RSV cases 84% from KSA birth cohort |
Distribution of RSV MALRTIs by health event over the first RSV season of KSA infants

 |
SAR ~607 million Direct economic burden of RSV in infants |
Distribution of RSV MALRTIs by related direct medical costs over the first RSV season of KSA infants
Percentages may not add to 100% due to rounding. All costs are in 2021 United States dollars.
ED, emergency department; ICU, intensive care unit; MV, mechanical ventilation; LRTI, lower respiratory tract illness; MA, medically attended; RSV, respiratory syncytial virus; SoC, standard of care; US, United States.
Red Flags
|
 |
Results
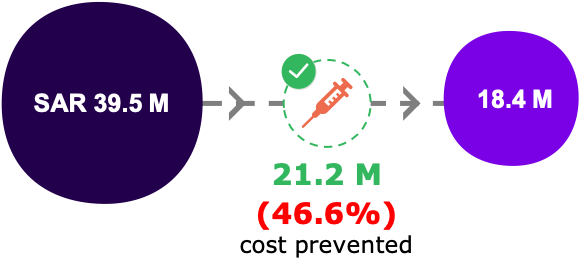
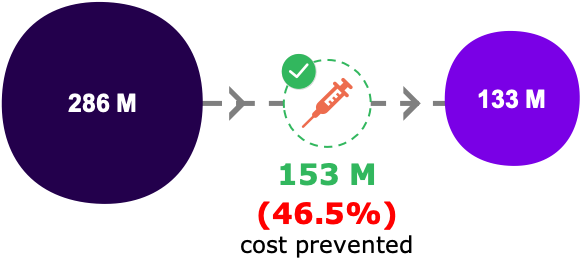
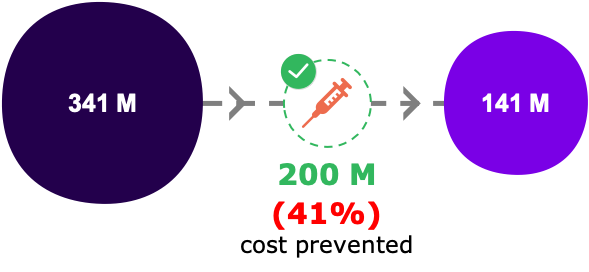
Impact of LA mAb for all KSA infants
Cases Vs budget saving
|
RSV-related health events |
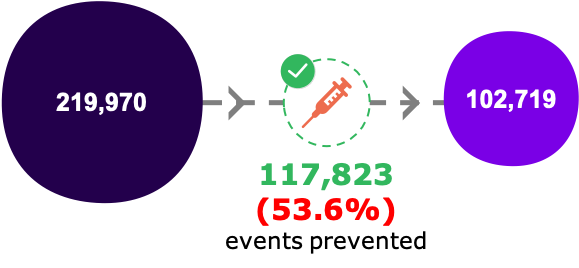
Primary Care Visits
|
ER Visits
|
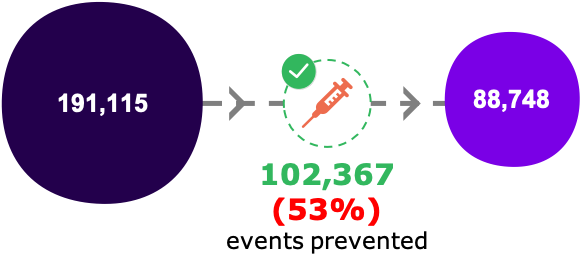
Hospitalizations*
|
|
Direct costs saving (374 millions)
|
|
|
|
| Reduce RSV cases by more than 50% and associated healthcare costs by more than 60% | |||
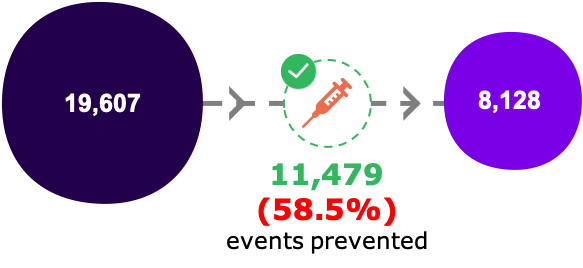
*Includes hospitalization that resulted in ICU admission or MV.
ED, emergency department; ICU, intensive care unit; MV, mechanical ventilation; RSV, respiratory syncytial virus; US, United States.
