Saudi initiatives on Bronchiolitis Recommendations
The first choice of RSV prevention is Nirsevimab;
alternatively, palivizumab is to be considered in case of unavailability of Nirsevimab.
 |
Eligibility considerations regarding Nirsevimab were as follows:
|
The SIBRO panel recommends RSV mAb as a prevention strategy that should be inserted into routine immunization calendars
RSV: Respiratory syncytial virus; mAb: monoclonal antibody
Alharbi, A. S., Alqwaiee, M., Al-Hindi, M. Y., Mosalli, R., Al-Shamrani, A., Alharbi, S., Yousef, A., Al Aidaroos, A., Alahmadi, T., Alshammary, A., Miqdad, A., Said, Y., & Alnemri, A. (2018). Bronchiolitis in children: The Saudi initiative of bronchiolitis diagnosis, management, and prevention (SIBRO). Annals of thoracic medicine, 13(3), 127–143. https://doi.org/10.4103/atm.ATM_60_18
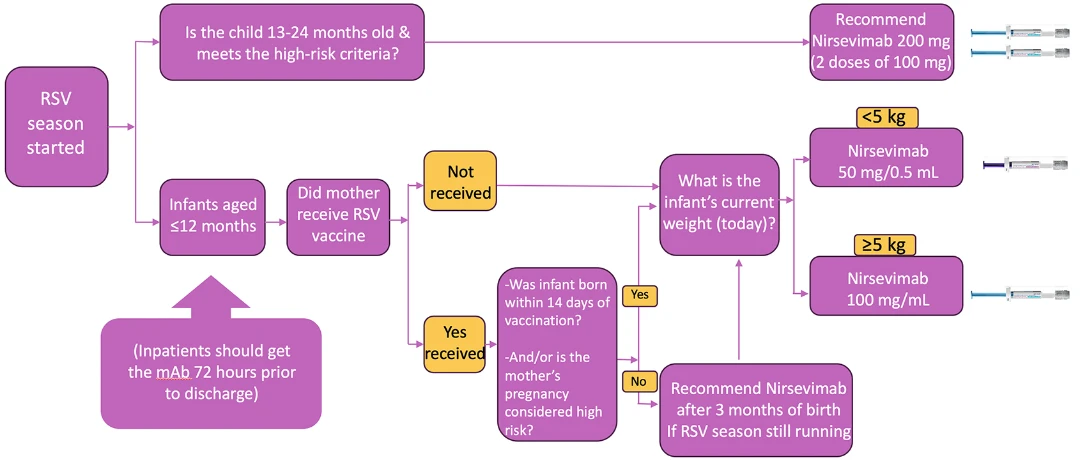
Saudi Initiative of Bronchiolitis Diagnosis, Management, and Prevention (Nirsevimab administration guide)
RSV: Respiratory syncytial virus; mAb: monoclonal antibody
Alharbi, A. S., Alqwaiee, M., Al-Hindi, M. Y., Mosalli, R., Al-Shamrani, A., Alharbi, S., Yousef, A., Al Aidaroos, A., Alahmadi, T., Alshammary, A., Miqdad, A., Said, Y., & Alnemri, A. (2018). Bronchiolitis in children: The Saudi initiative of bronchiolitis diagnosis, management, and prevention (SIBRO). Annals of thoracic medicine, 13(3), 127–143. https://doi.org/10.4103/atm.ATM_60_18
| Recommendations for Nirsevimab Immunoprophylaxis | |||
| *The recommended interval between the last dose of palivizumab and a dose of Nirsevimab (in High-risk Infants) is 1 month (similar to the interval if the infant were to receive another dose of palivizumab).[5] | |||
| & The recommendations for Nirsevimab for high-risk children apply to infants and children recommended to receive palivizumab. [1] | |||
|
|||
|
# Maternal vaccination efficacy is not established in:
|
|||
| @ High-risk infants who are hospitalized or still in NICU during the season should get the recommended schedule. Also, eligible infants at the beginning of the season and ready for discharge from NICU should receive the first dose up to 72 hours prior to discharge. [28] | |||
| ^The mAb included Palivizumab & Nirsevimab does not interfere with the immune response to live or inactivated vaccines. The childhood immunization schedule should be followed for all children, regardless of mAb use [30] | |||
| Intramuscular (IM) injection Use a 22–25-gauge needle. [5] | Age | Needle length | Injection site |
| Newborns (1st 28 days) | ⅝"a | Anterolateral thigh muscle | |
| Infants (1–12 months) | 1" | Anterolateral thigh muscle | |
| Toddlers (1–2 years) | 1–1¼" | Anterolateral thigh muscle c | |
| ⅝b–1" | Deltoid muscle of arm | ||
RSV=Respiratory syncytial virus, CLD=Chronic lung disease, IM=Intramuscular, mAbs=Monoclonal antibodies, NICU=Neonatal intensive care unit
|
Considerations for high-risk infants
|
 |
RSV: Respiratory syncytial virus
Alharbi, A. S., Alqwaiee, M., Al-Hindi, M. Y., Mosalli, R., Al-Shamrani, A., Alharbi, S., Yousef, A., Al Aidaroos, A., Alahmadi, T., Alshammary, A., Miqdad, A., Said, Y., & Alnemri, A. (2018). Bronchiolitis in children: The Saudi initiative of bronchiolitis diagnosis, management, and prevention (SIBRO). Annals of thoracic medicine, 13(3), 127–143. https://doi.org/10.4103/atm.ATM_60_18
