.2024-04-18-12-59-18.png)

DUPIXENT is the first-line systemic choice for achieving lasting change in patients as young as 6 years old with atopic dermatitis*
*DUPIXENT is indicated to treat adults and adolescents with moderate-to-severe atopic dermatitis, and children aged 6 years to 11 years old with severe atopic dermatitis who are candidates for systemic therapy1
- DUPIXENT Summary of Product Characteristics. August 2023
MODERATE-TO-SEVERE ATOPIC DERMATITIS IS A CHRONIC, DEBILITATING INFLAMMATORY DISEASE THAT REQUIRES LONG-TERM CONTROL1

Nour, 28

Frustrated with recurrent disease
exacerbations despite using her
topical treatments
Topical + oral corticosteroids

Khalid, 16
Experiences persistent lesions and itch
TCS + immunosuppress-ant

Farah, 7
Wakes up at night due to intense itching
TCS + topical calcineurin inhibitors
Bader, 32
Experiences recurrent disease exacerbations
TCS

Abeer, 65
Experiences persistent disease
TCS + immunosuppress-ant
Illustrative patient profiles, not actual patients.
- Leung DYM et al. J Clin Invest 2004; 113:651—657.
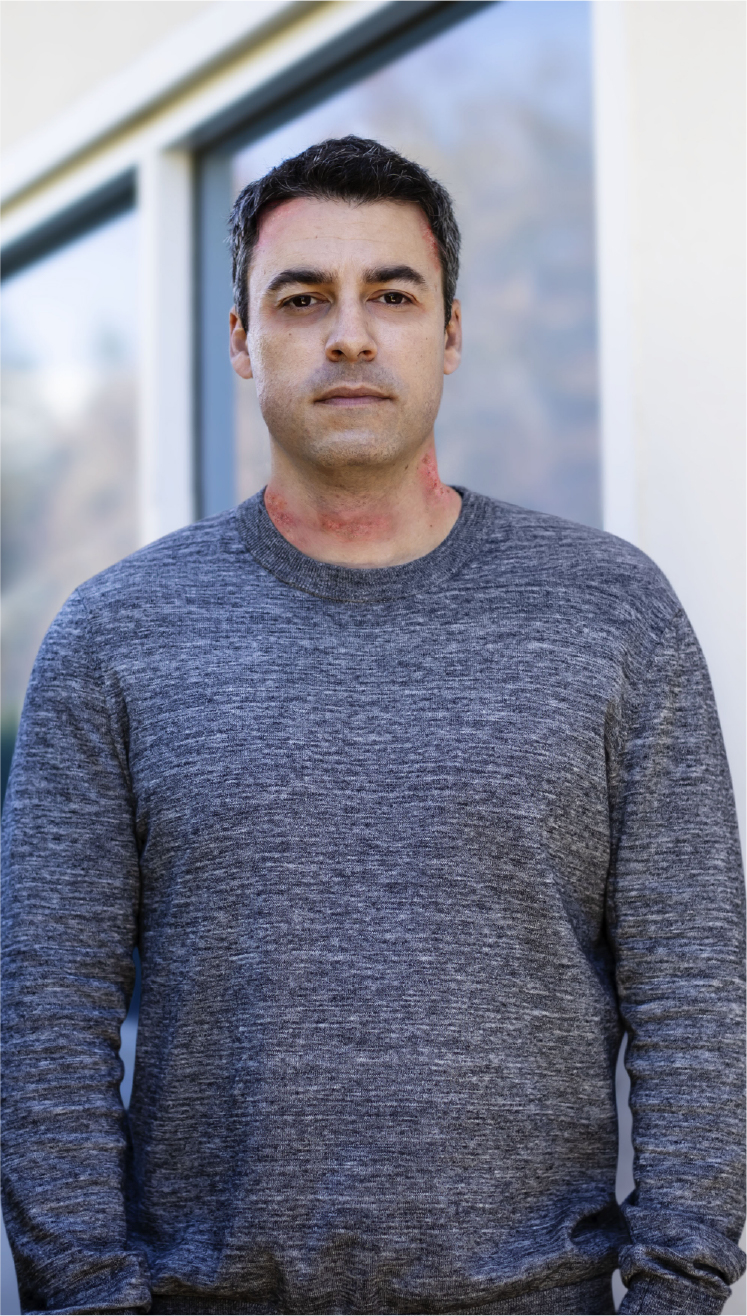
NOUR, 28
“I’ve had this disease since I was a child. I’ve tried countless topical treatments and my skin is still sore and itchy. What’s the point?”
About Nour
 Works in retail
Works in retail
Diagnosed with atopic dermatitis as a child
Inadequately controlled with TCS
- Painful lesions in flexural areas, erythema, and edema
- Recurring, uncontrolled flares
Impact on QoL
Missed several work days and worried about career progression
Unable to focus at work due to itch disrupting sleep
Avoids exercise and clothes that expose arms or legs
Wants to have a baby but is worried about the effects of her treatment on the baby
Treatment
Longstanding history of medium-to-high potency TCS with intensive and time-
consuming application regimen
Occasional oral corticosteroids – experienced temporarily altered mood and bruising easily
Goals
Develop her career in the retail industry
Have a baby in the near future
Desperate to control her atopic dermatitis so that she can live her life fully
Illustrative patient profile, not actual patient
KHALID, 16
"The lesions on my face are the worst. I wish they would go away”
About Khalid
High school student
Enjoys sports
Diagnosed with atopic dermatitis at 8 years old
Inadequately controlled despite TCS
- Lesions in high impact areas
- Dry skin, chronic pruritus, and skin erosions
Impact on QoL
Seven prolonged school absences this year and grades have fallen
Unable to concentrate at school as itch interrupts sleep
Worried about exams and atopic dermatitis limiting his course choice at university
Self-conscious about his skin so avoids socializing
Parents are worried about the effect of atopic dermatitis on Khalid and his education
Treatment
Frequent medium-to-high potency TCS
Immunosuppressant treatment – Stopped early as muscle weakness experienced
Goals
Go to university
Socialize more like his friends do
Start dating
Find a treatment that does not need to be administered daily
Like his parents, George wants to focus on school rather than on his disease

Illustrative patient profile, not actual patient
FARAH, 7
"My skin really hurts, it’s so itchy I can’t sleep at night”
About Farah
Diagnosed with atopic dermatitis at 1 year old
Inadequately controlled with TCS and topical calcineurin inhibitors
- Chronic lesions on neck and across the body
- Frequent worsening of disease
Impact on QoL
Missed school days causing her parents to miss work
Cries at night as she is unable to sleep due to itching
Feels isolated from her classmates and anxious about her atopic dermatitis
Parents are worried about the impact of missing school on her development
Treatment
Has not achieved control of her disease since diagnosis
Medium-to-high potency TCS and topical calcineurin inhibitors
Goals
Wants the itching and lesions to go away
Wants to go to school and see her friends
Parents want to find a treatment that works and is safe for longterm use
Parents don’t want her life choices to be restricted by her atopic dermatitis
llustrative patient profile, not actual patient
- Irvine AD and Mina-Osorio P. Br J Dermatol 2019; 181:895–906.
- Margolis JS et al. JAMA Dermatol 2014; 150(6):593–600.
PATIENTS WANT THEIR DISEASE UNDER CONTROL, WHATEVER THEIR AGE
The continuous burden of atopic dermatitis can have far-reaching impact on the QoL of patients and their families1–3

70%
experience sleep loss. 5* In general, sleep loss can have a negative effect on neurocognitive performance6
20%
miss school because of the disease5*
86%
avoid everyday activities, and over 50% feel unhappy or depressed2

38%
alter their educational or career trajectory due to the disease7
80
nights of sleep a year can be
impacted by the disease in adults2
12
weeks of work productivity are lost per year due to disease in adults8
64%
experience problems at work including itch, fatigue, pain, and psychological complaints9
THE BURDEN OF INADEQUATELY CONTROLLED ATOPIC DERMATITIS MAY BECOME CUMULATIVE AND IMPACT PATIENTS THROUGHOUT THEIR LIVES1-3
*The age of children included in the Eczema Society of Canada Atopic Dermatitis Quality of Life Report survey ranged from 0 to 18 years.
PATIENTS WITH ATOPIC DERMATITIS MAY NEED A TREATMENT THEY CAN RELY ON FOR THE LONG-TERM
Atopic dermatitis has a highly fluctuating and unpredictable course of disease1
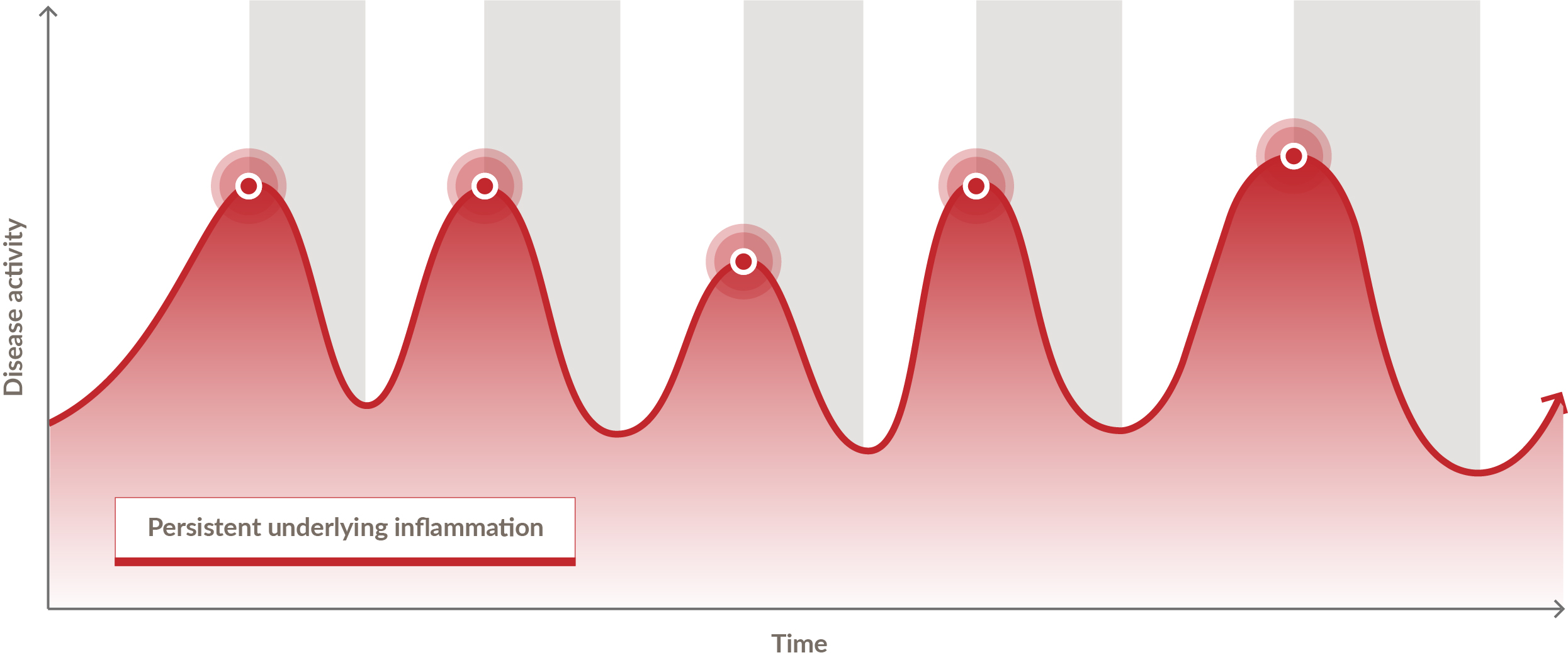
 A chronic, inadequately controlled
A chronic, inadequately controlled
disease driven by persistent
underlying inflammation2,3
 Patients may experience
Patients may experience
intensified disease activity for 30–
50% of the year4
 Treatment using a reactive, episodic approach does not address the fluctuating and unpredictable nature of atopic dermatitis1,5
Treatment using a reactive, episodic approach does not address the fluctuating and unpredictable nature of atopic dermatitis1,5
- Bieber T. Nat Rev Drug Discov. 2022; 21(1):21–40.
- Gittler J et al. J Allergy Clin Immunol 2012; 130:1344–1354.
- Guttman-Yassky E et al. J Allergy Clin Immunol 2011; 127:1420–1432.
- Zuberbier T et al. J Allergy Clin Immunol 2006; 118:226–232.
- Leung DYM et al. J Clin Invest 2004; 113:651–657.
PATIENTS WITH ATOPIC DERMATITIS MAY NEED A TREATMENT THEY CAN RELY ON FOR THE LONG-TERM
For proactive and continuous control of their underlying inflammation1
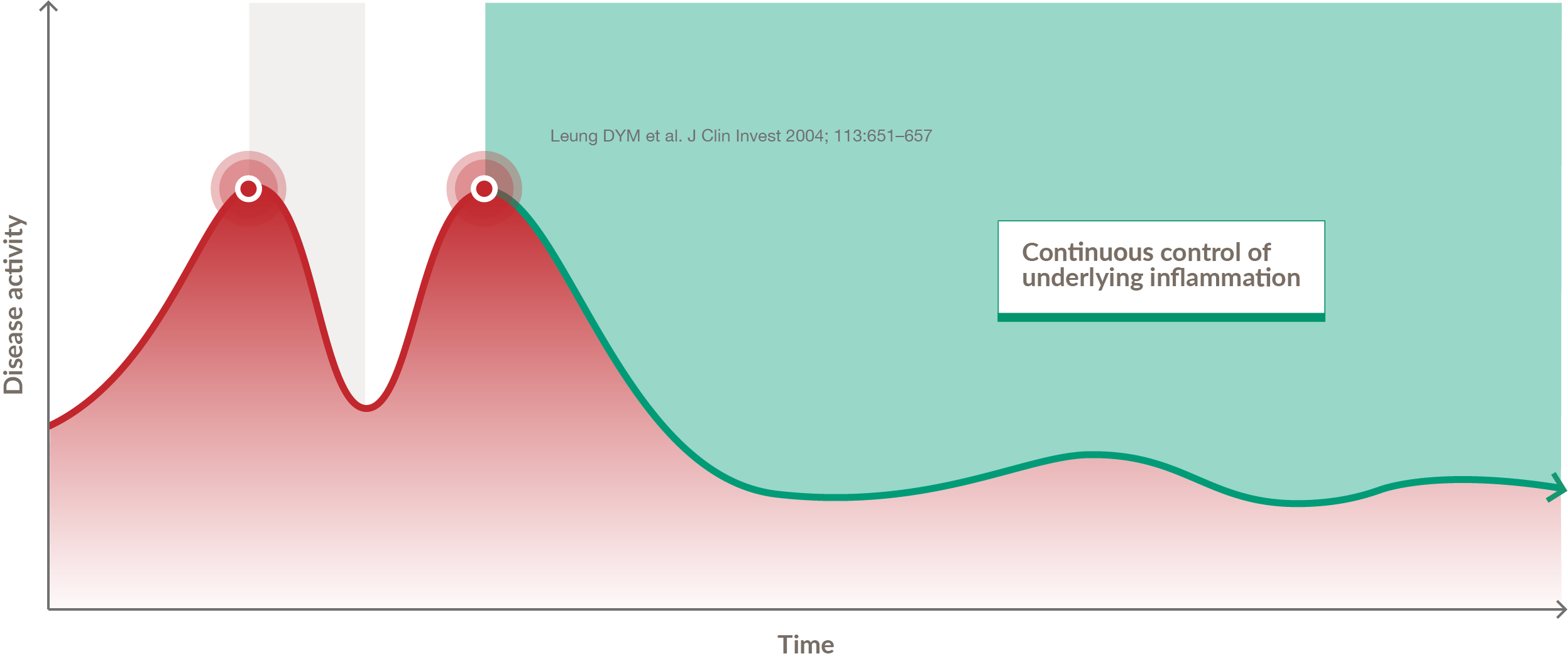
 A more sustainable treatment paradigm proactively targets the persistent underlying inflammation with a safety profile that allows for continuous treatment2-4
A more sustainable treatment paradigm proactively targets the persistent underlying inflammation with a safety profile that allows for continuous treatment2-4
 Adequately controlled disease with
Adequately controlled disease with
long-term improvements in signs,
symptoms, and QoL
- Leung DYM et al. J Clin Invest 2004; 113:651–657.
- Wollenberg A et al. J Eur Acad Dermatol Venereol 2018; 32(6):850–878.
- Wollenberg A et al. Ann Dermatol 2012; 24(3):253–260.
- Wollenberg A et al. J Eur Acad Dermatol Venereol 2018; 32(5):657–682.
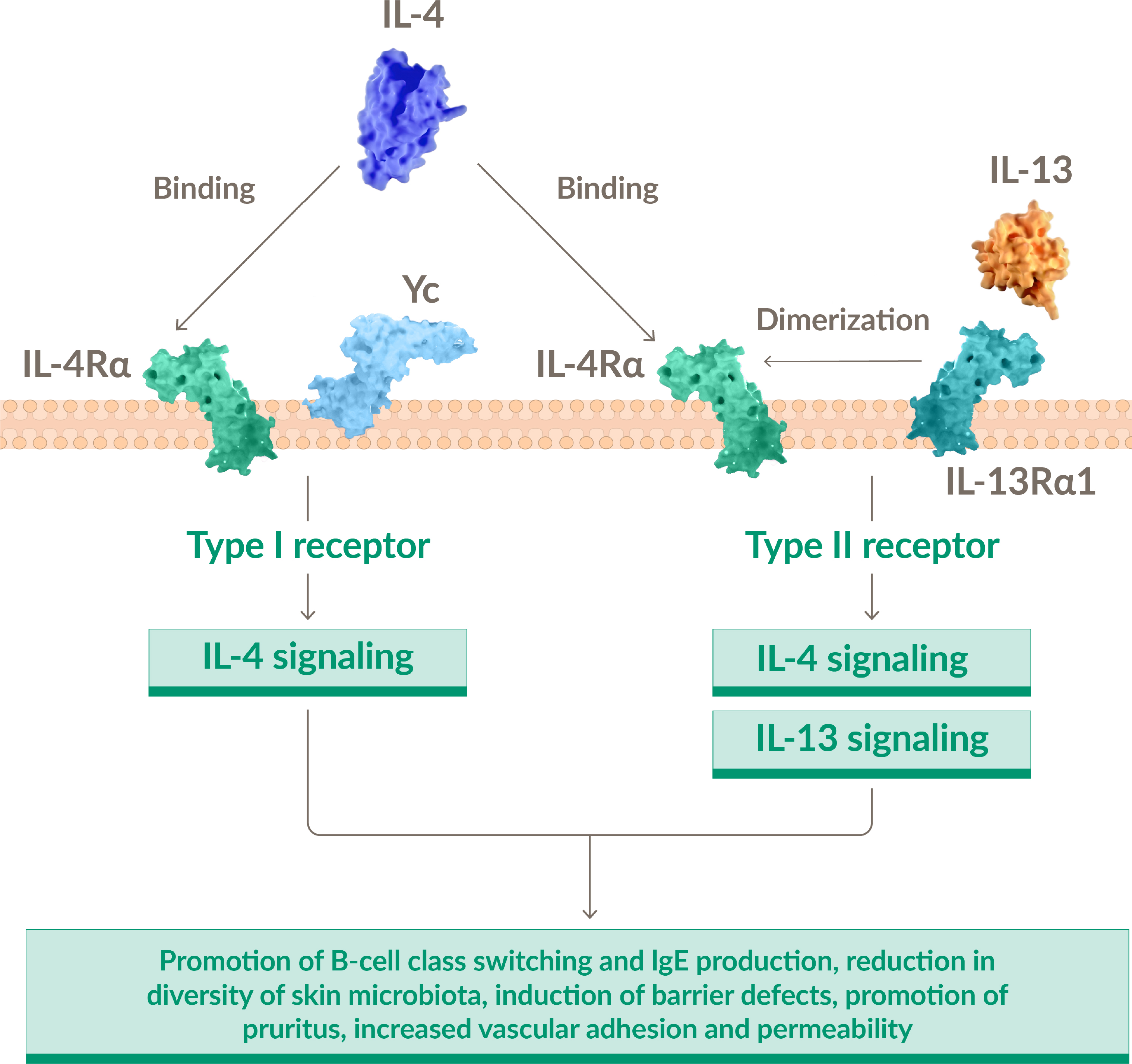
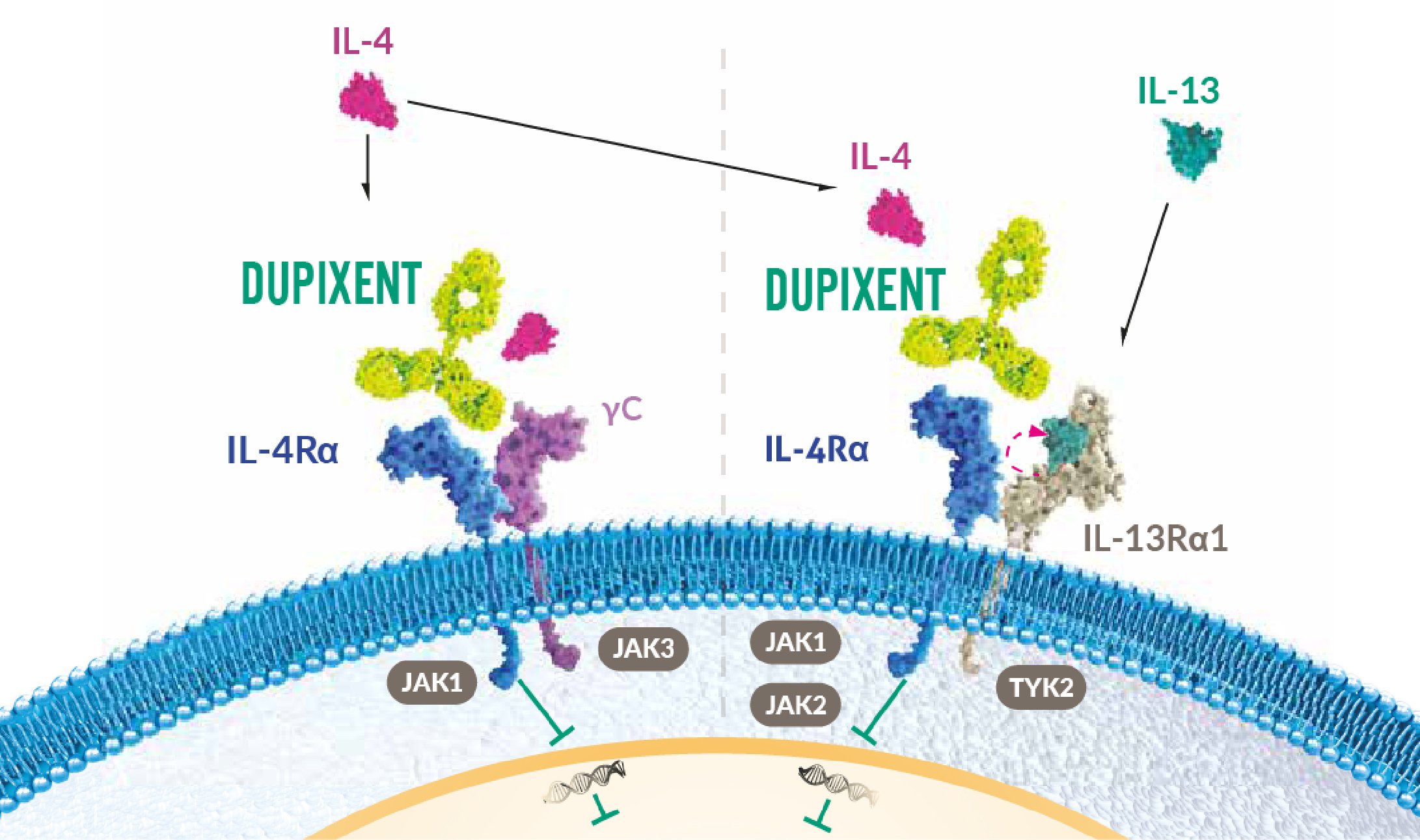
IL-4 AND IL-13 ARE TWO KEY MEDIATORS OF TYPE 2 INFLAMMATION AND IMPACT SKIN BARRIER DYSFUNCTION1,2
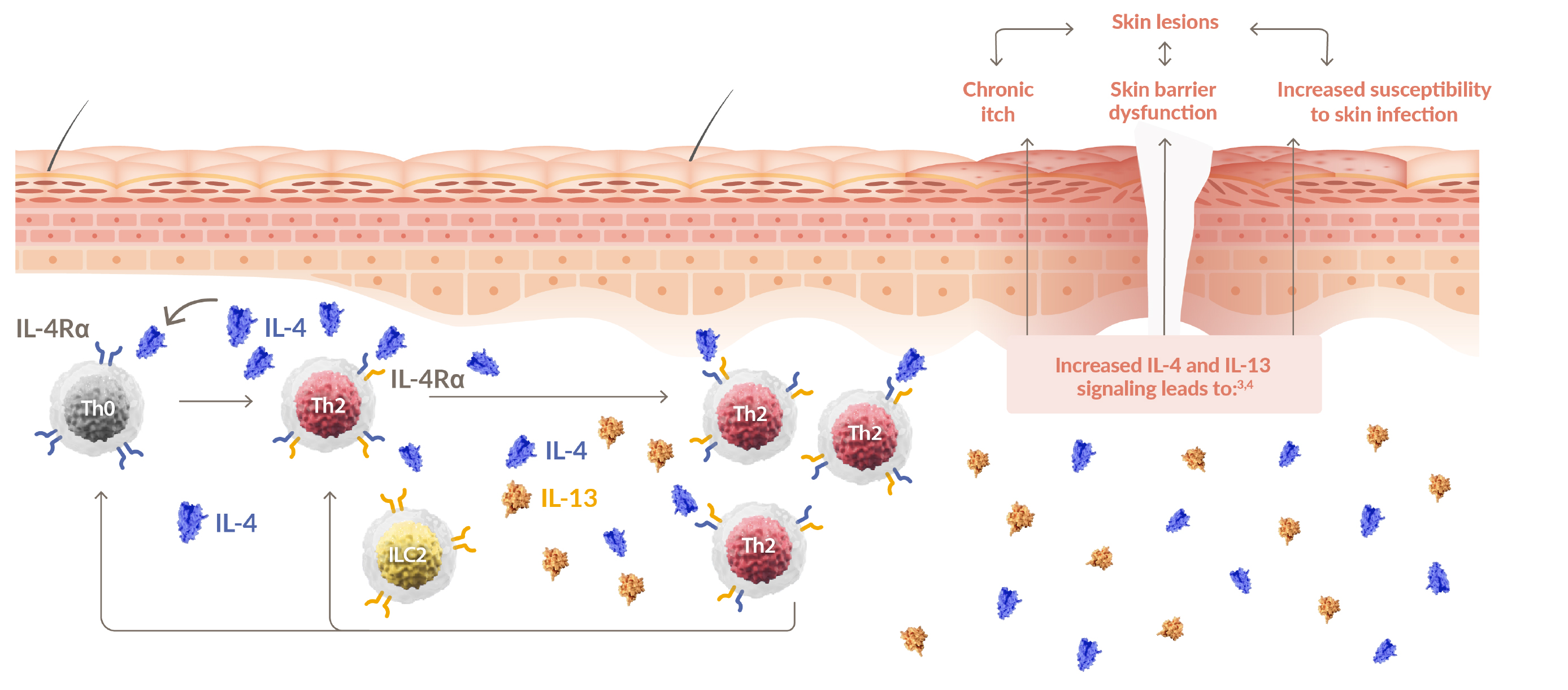
 IL-4 is the central driver of Th2 cell differentiation and
IL-4 is the central driver of Th2 cell differentiation and
activation2
IL-4 creates a feedback loop, which perpetuates the inflammatory process2
IL-4 AND IL-13 HAVE OVERLAPPING FUNCTIONS, BUT IL-4 HAS AN EXCLUSIVE ROLE5
IL-4 and IL-13 both mediate inflammation and barrier dysfunction but only IL-4 promotes differentiation of Th cells from Th0 to Th25
NONLESIONAL SKIN IS NOT NORMAL SKIN
In atopic dermatitis, subclinical inflammation is also present in nonlesional skin1,6,7
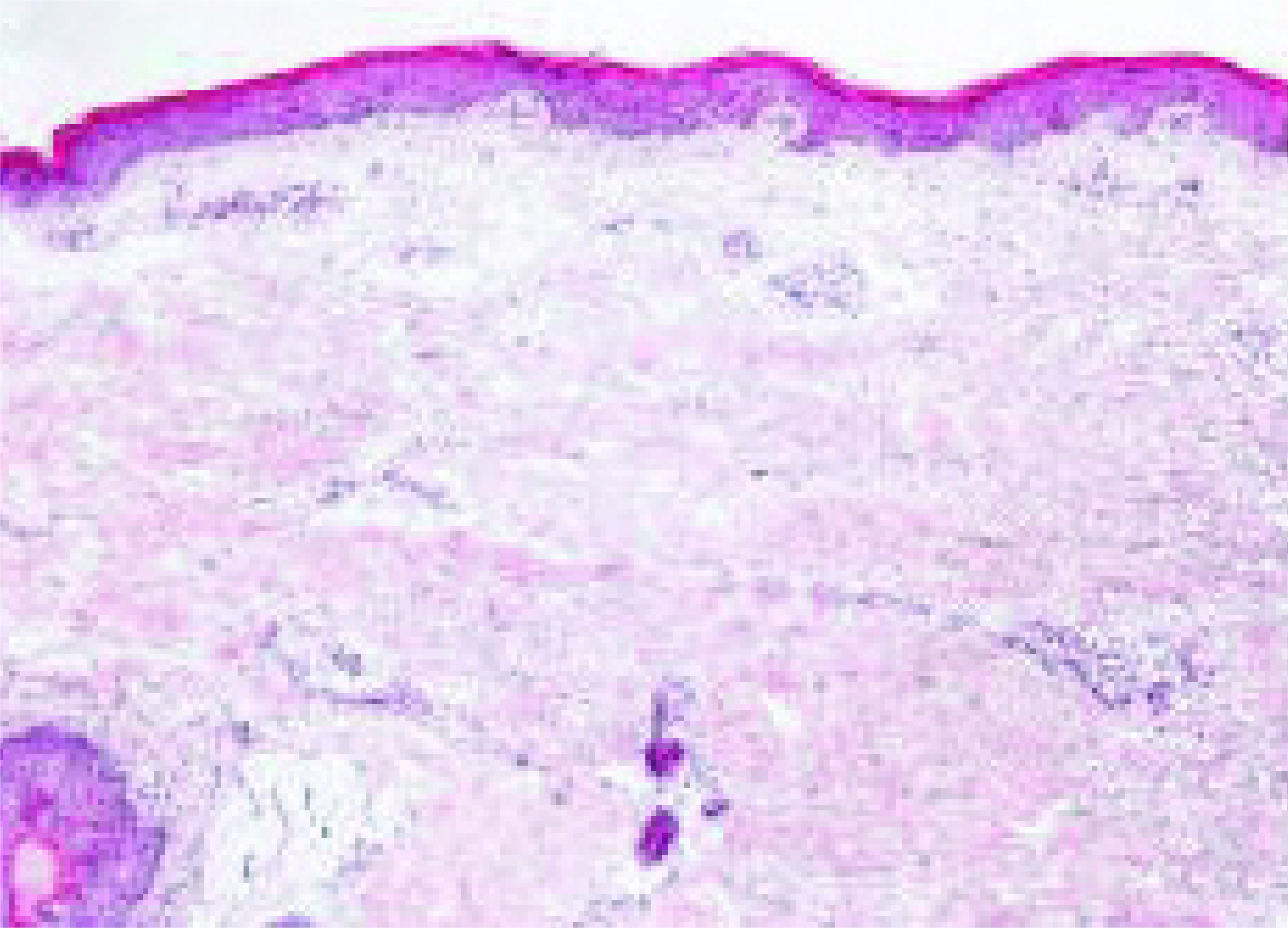
Normal skin
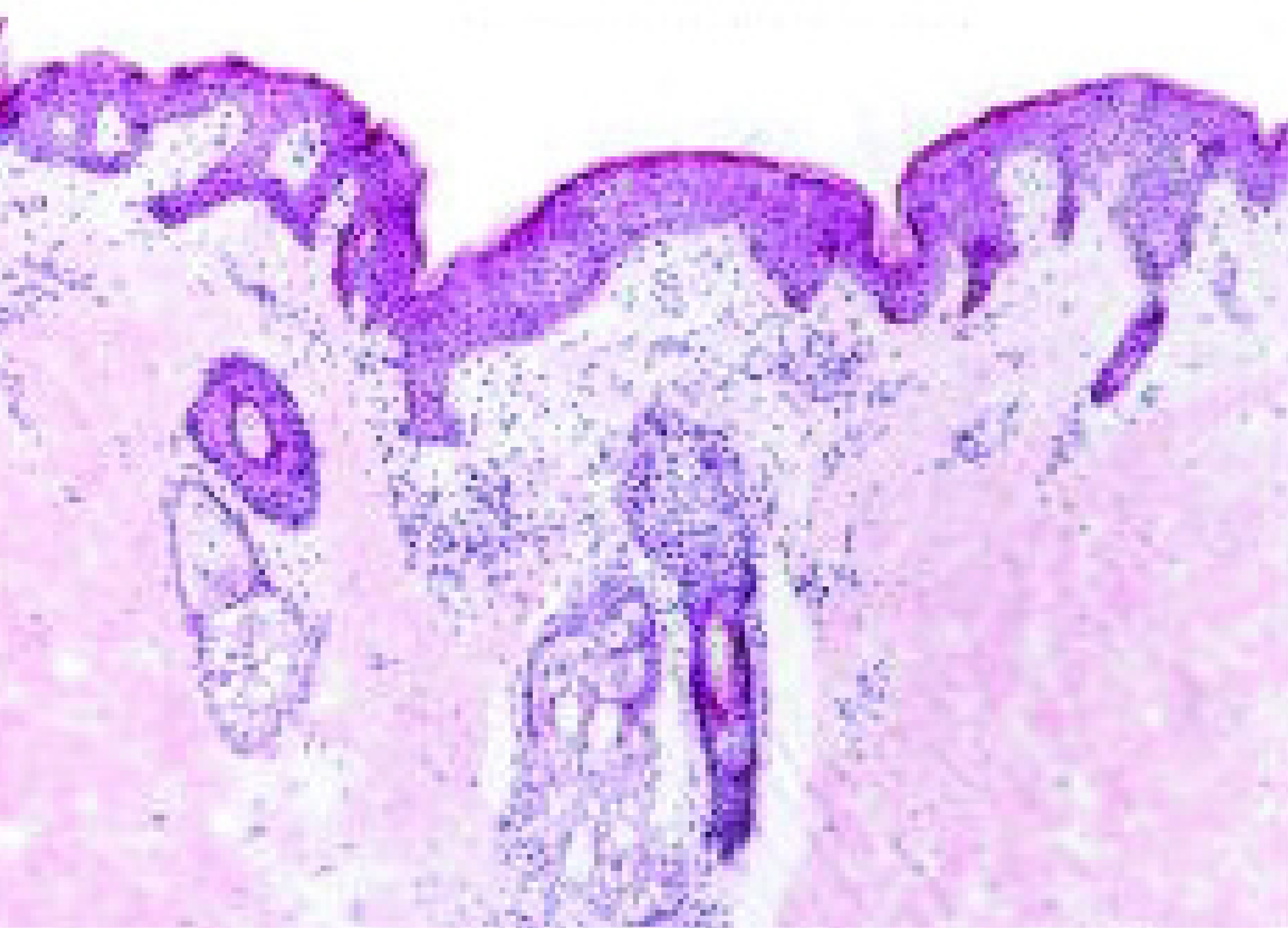
Nonlesional skin
- Gittler JK et al. J Allergy Clin Immunol 2012; 130:1344–1354.
- Capozza K et al. Dermatitis 2020;31(3): 223–227.
- Biedermann T et al. Front Immunol 2015; 6:353.
- Rerknimitr P et al. Inflamm Regen 2017; 37:14.
- Beck L et al. JID Innova ons 2022; doi: https://doi.org/10.1016/j.xjidi.2022.100131.
- Gandhi NA et al. Nat Rev Drug Discov 2016; 15:35–50.
- Artis D and Spits H. Nature 2015; 517:293–301.
DUPIXENT IS THE FIRST AND ONLY TARGETED IMMUNOMODULATOR TO SPECIFICALLY TARGET TWO KEY MEDIATORS OF TYPE 2 INFLAMMATION, IN THE PATHOPHYSIOLOGY OF ATOPIC DERMATITIS - IL-4 AND IL-131,2
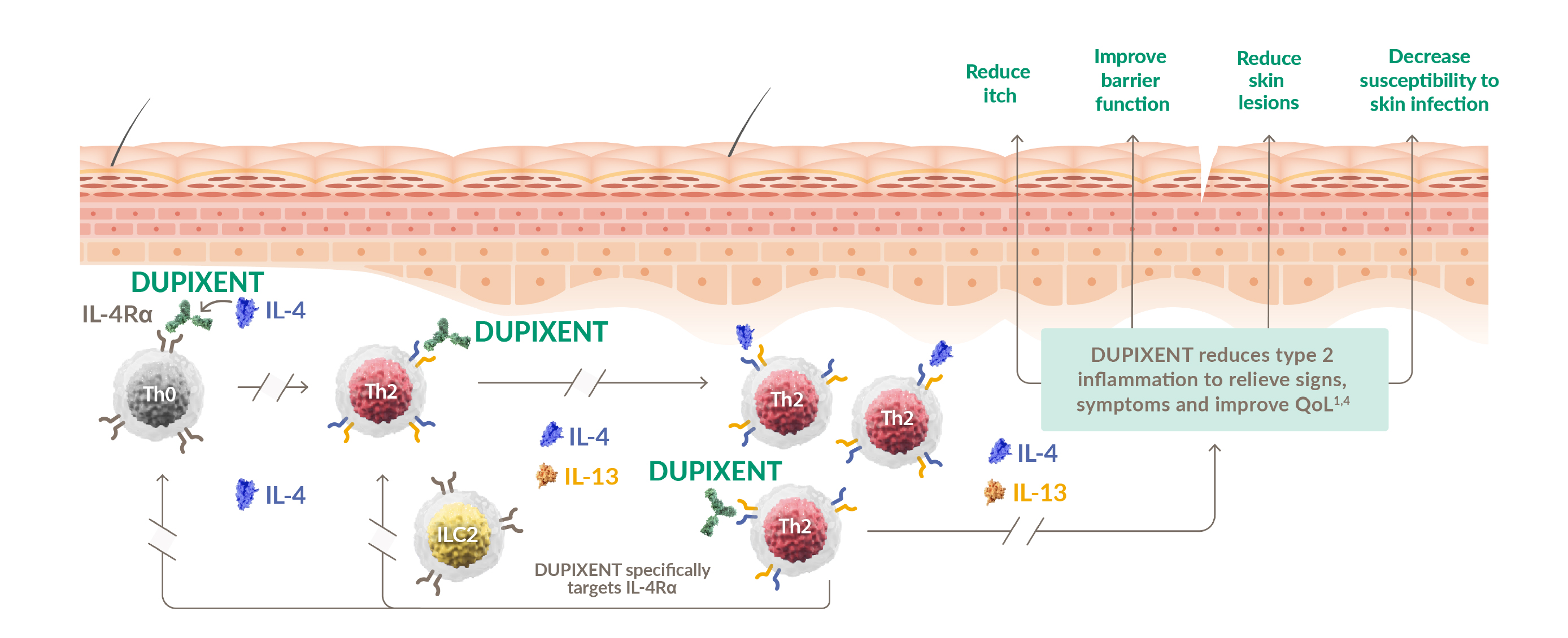

DUAL INHIBITION OF BOTH IL-13 AND IL-4 BY TARGETING A SINGLE RECEPTOR IL-4R (IL-4Rα)1
DUPIXENT is not an immunosuppressant1

RAPID AND SUSTAINED CONTROL AFTER THE FIRST DOSE1-4
Sustained improvement of itch, skin clearance, and QoL up to 52 weeks1–4
Rapid relief of itch and increased skin clearance, and QoL after the first dose1–4
Skin Clearance
65% of patients achieved EASI-75 at Week 521
~50% of patients achieved EASI-90 on DUPIXENT + TCS compared to ~15% with placebo + TCS at week 521*
Itch Relief
~60% mean percentage improvement in pruritus NRS score from baseline to Week 521,3
Quality of Life
80% of patients achieved a clinically meaningful improvement† in DLQI at Week 521,4

≥80%
response rate‡ based on improvements in lesions, itch, or QoL5
≥84%
of patients experienced no flares with DUPIXENT + TCS over 52 weeks (vs 57% with placebo + TCS)6
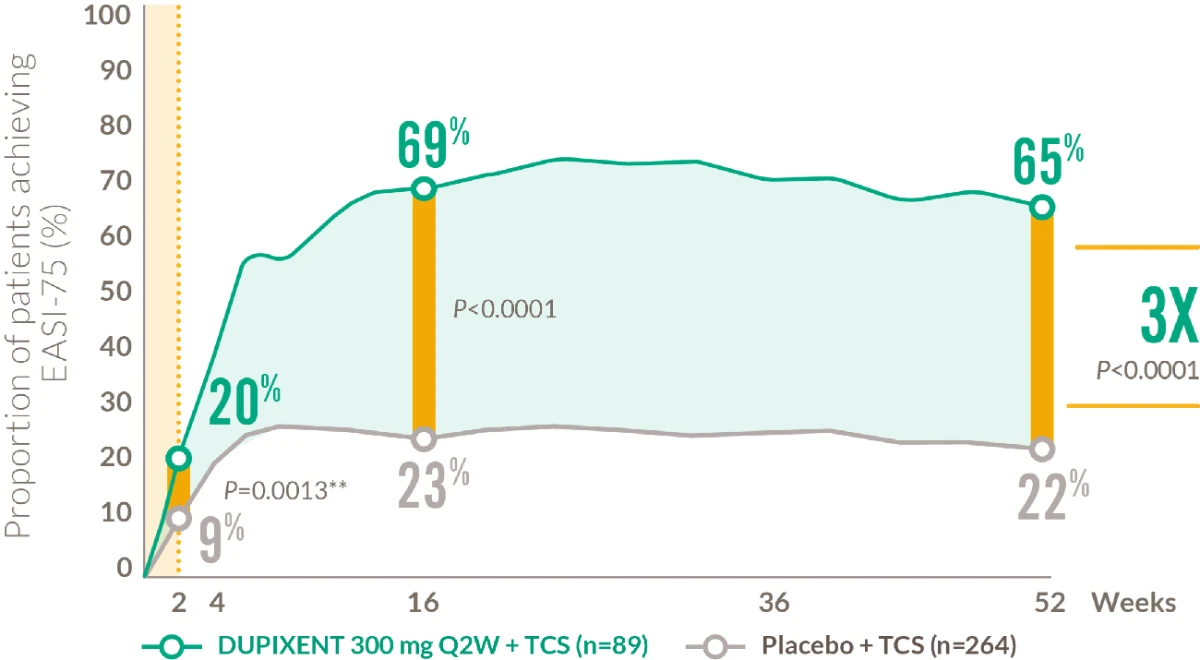
RAPID AND SUSTAINED IMPROVEMENT IN SKIN CLEARANCE AFTER THE FIRST DOSE1,2
18+ YEARS
Proportion of patients achieving EASI-75 from baseline to Week 521,2
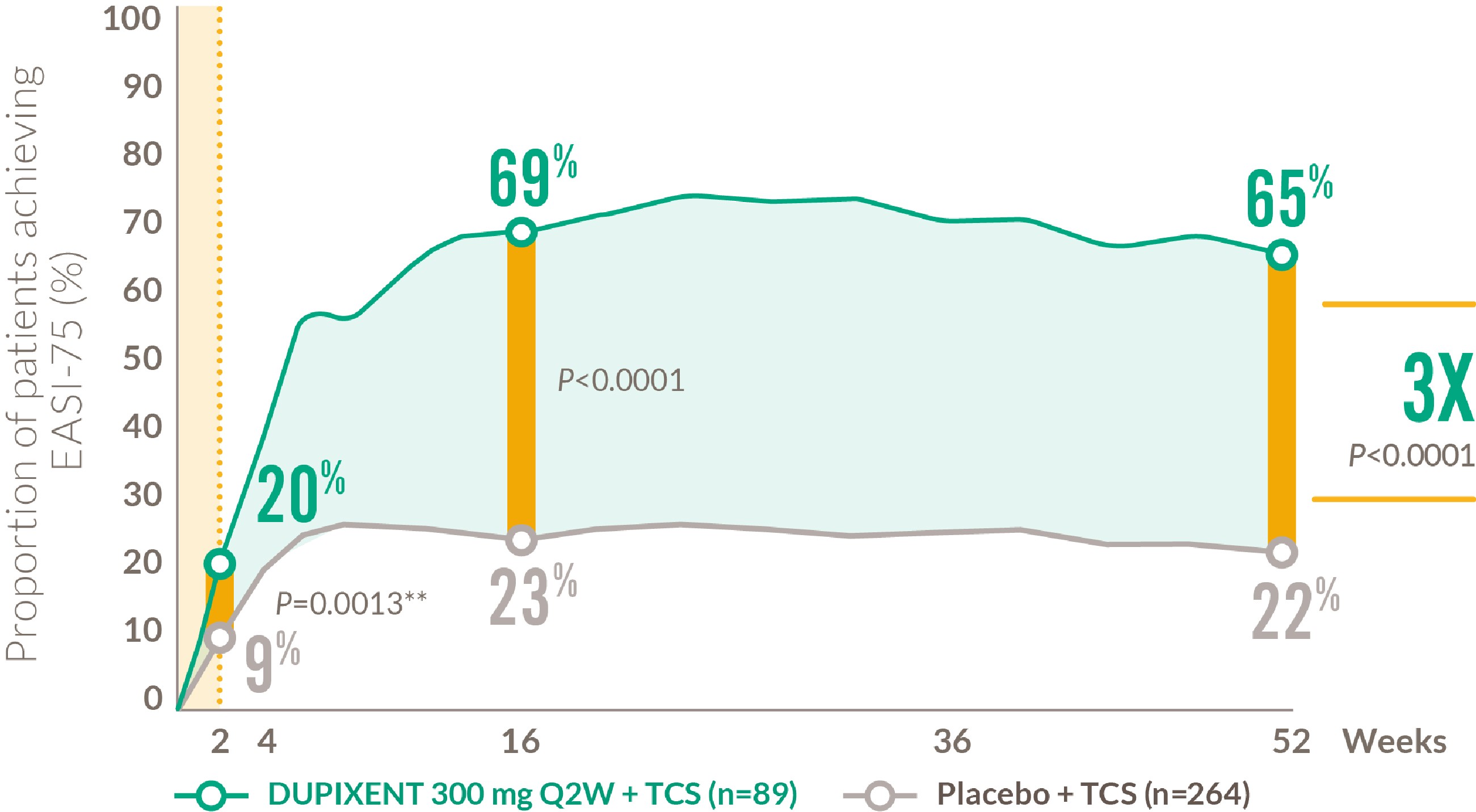
Coprimary endpoints in LIBERTY AD CHRONOS:2
-39% of DUPIXENT + TCS patients achieved IGA 0 or 1 vs 12% of placebo + TCS patients at Week 16
- 69% of DUPIXENT + TCS patients achieved EASI-75 vs 23% of placebo + TCS patients at Week 16
**Nominal P-value
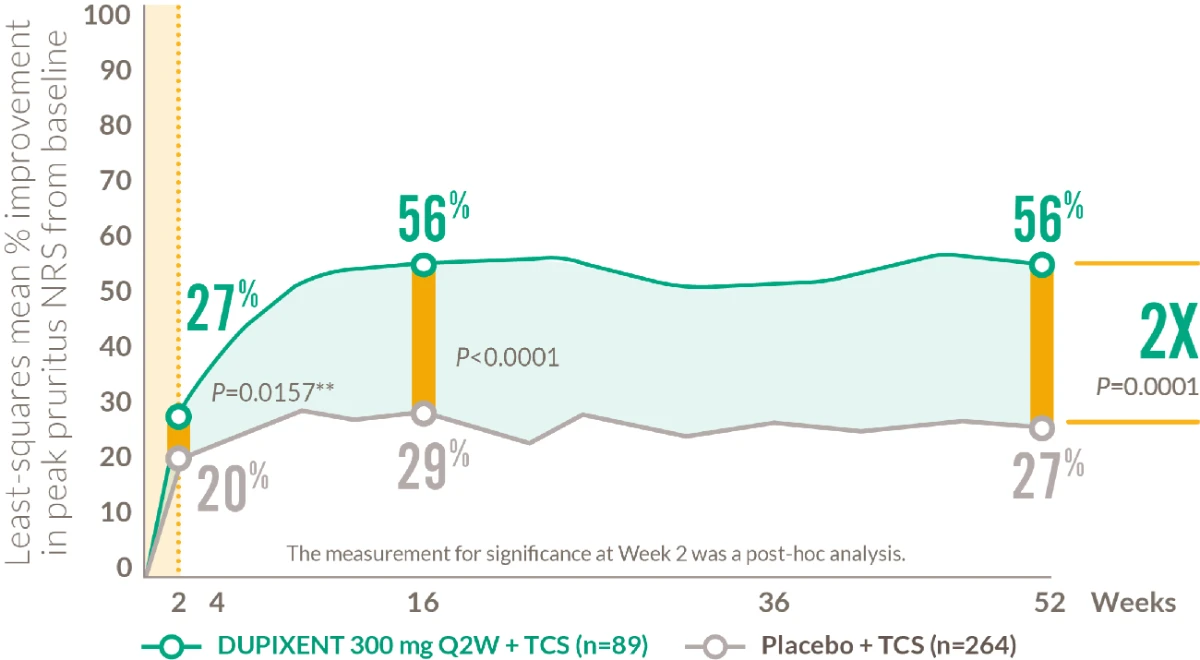
RAPID AND SUSTAINED IMPROVEMENT IN ITCH AFTER THE FIRST DOSE1,3
18+ YEARS
Mean percentage improvement in pruritus NRS score from baseline to Week 521,3
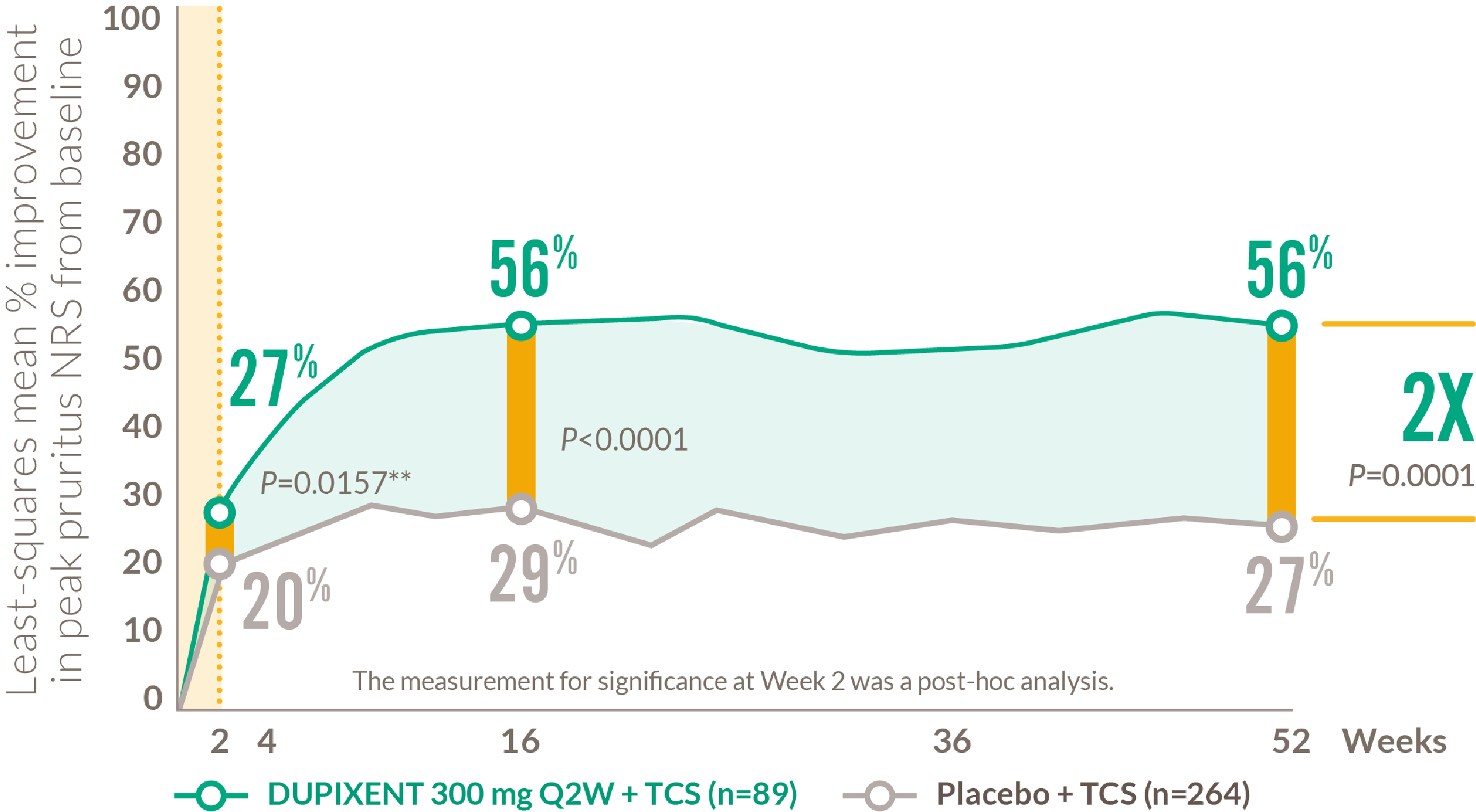
**Nominal P-value
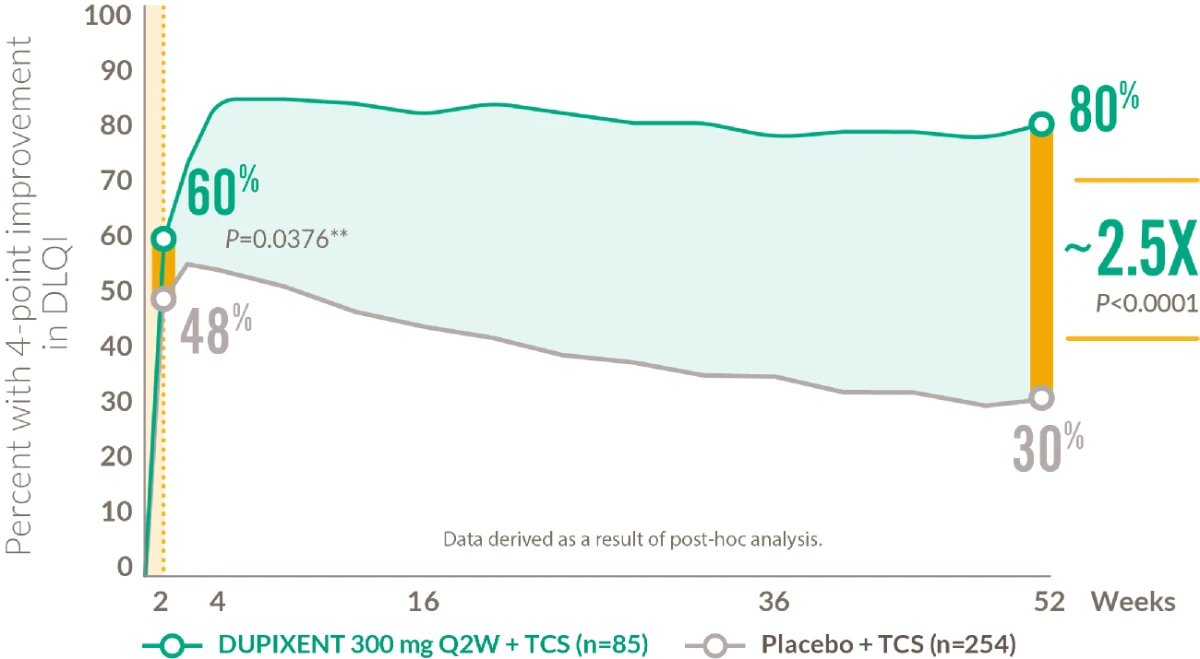
RAPID AND SUSTAINED IMPROVEMENT IN QUALITY OF LIFE AFTER THE FIRST DOSE1,4
18+ YEARS
Patients achieving clinically meaningful improvement* in DLQI1,4
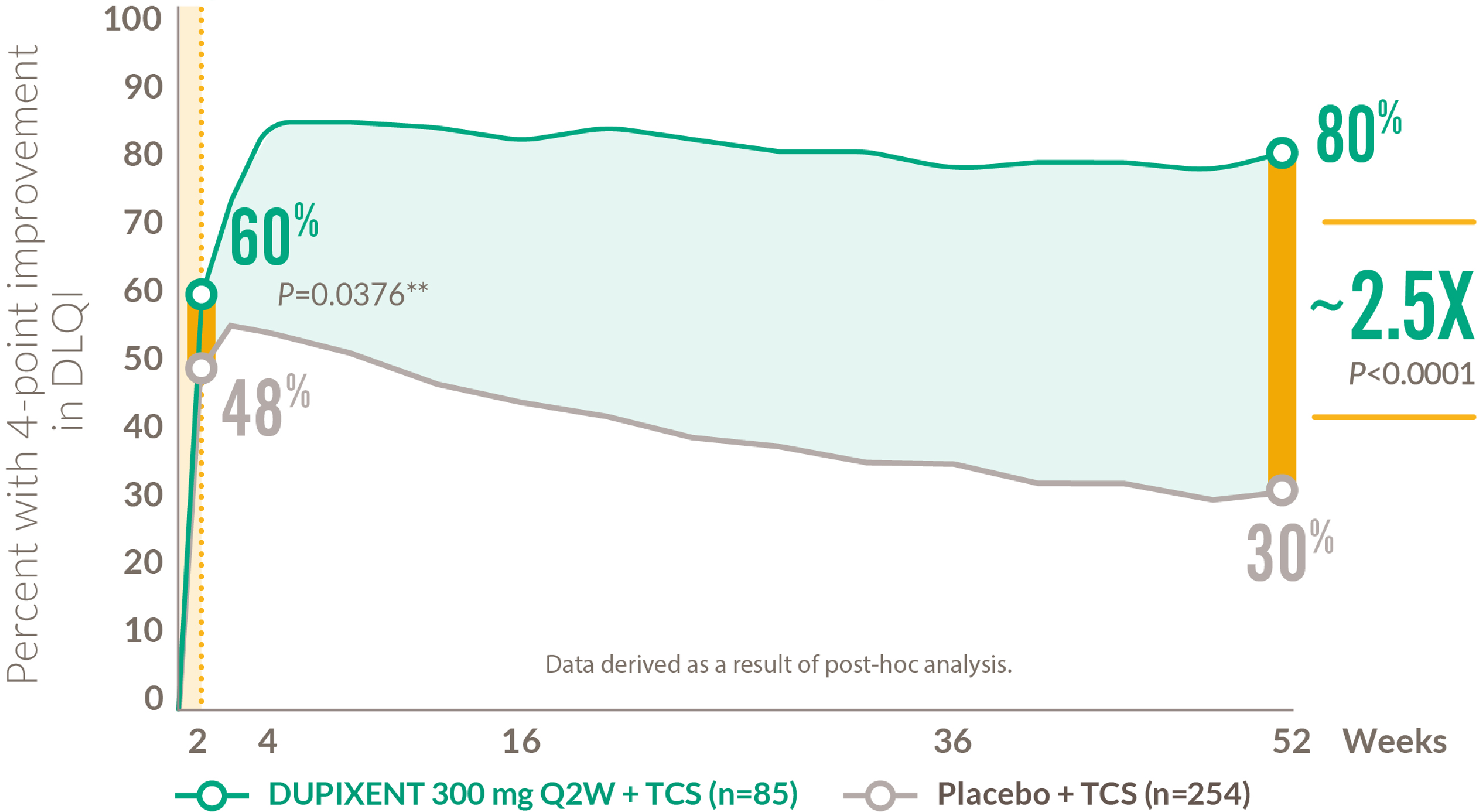
* Defined as a ≥ 4-point improvement in DLQI on a 0–30 point scale
**Nominal P-value
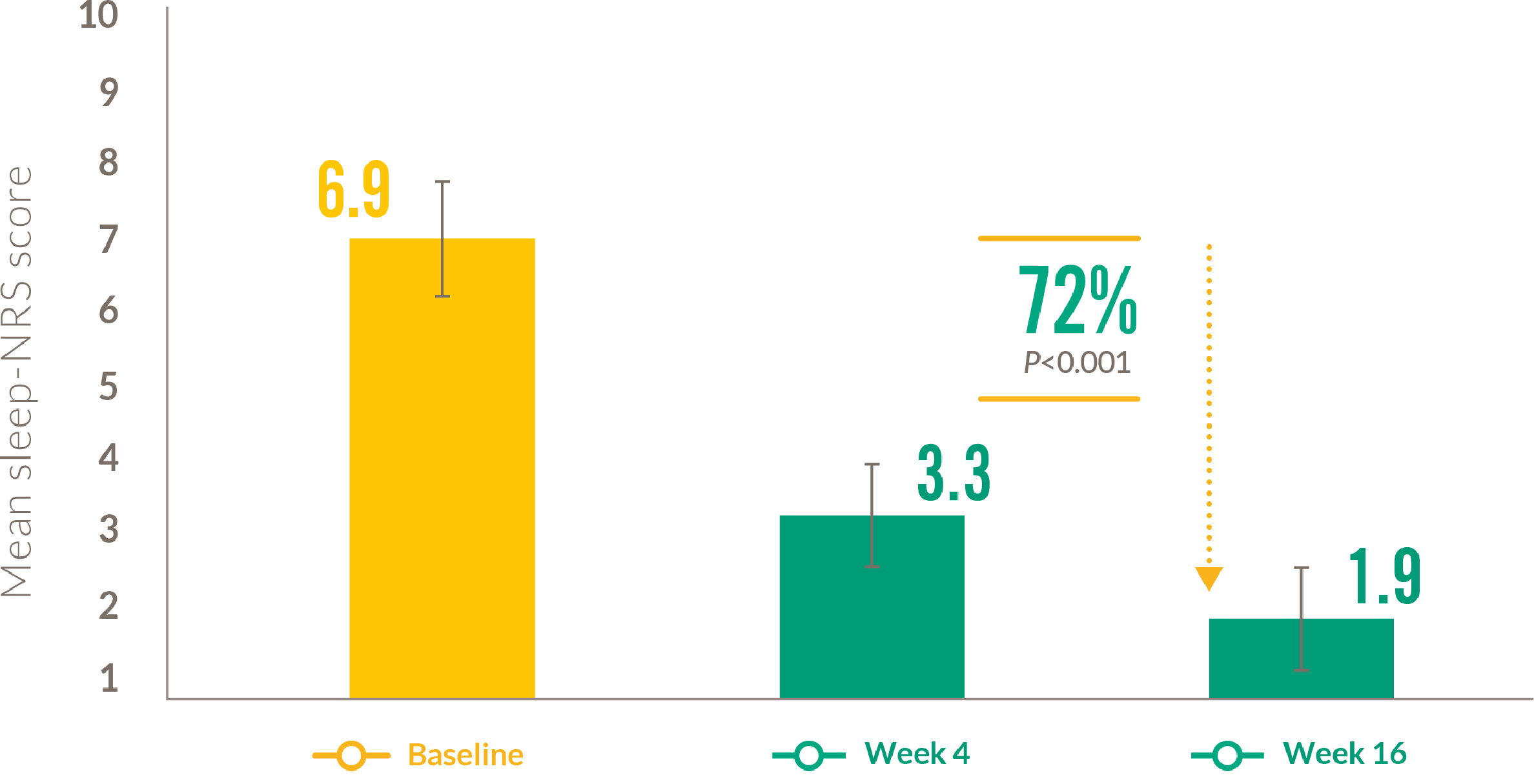
DUPIXENT REDUCED SLEEP LOSS7,8
18+ YEARS
Mean sleep NRS score with DUPIXENT from baseline to Week 16 7*
Patients who reported no days of sleep disturbance with DUPIXENT from baseline to Weeks 16 and 528**
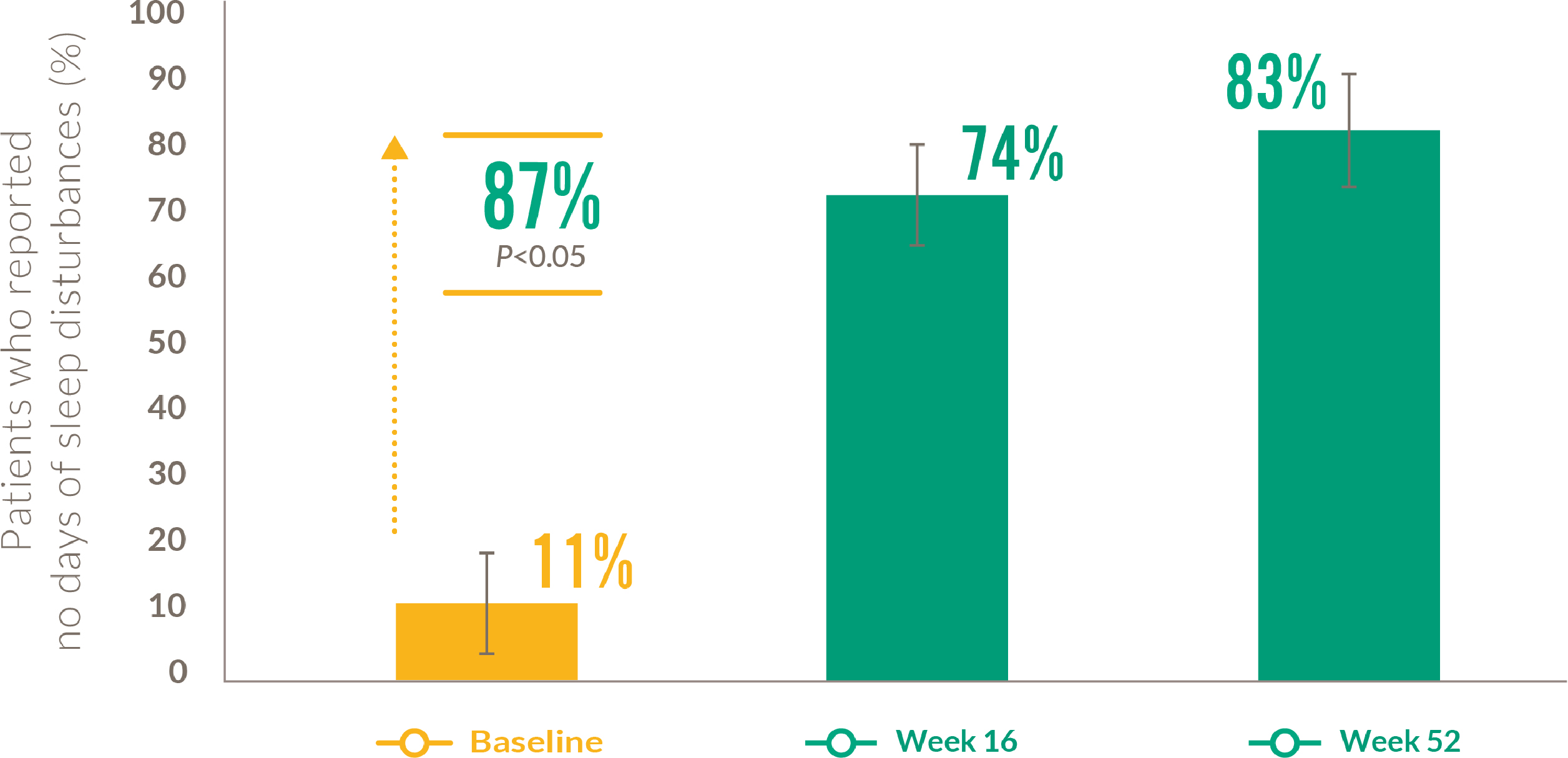
Sleep NRS is a single-item scale ranging from 0 (“best possible sleep”) to 10 (“worst possible sleep”)
*Retrospective, multicenter cohort study of adults with moderate-to-severe atopic dermatitis treated with DUPIXENT between June 2018 and February 2019 (N=109) from a national patient access program authorized by the Italian Medical Agency. Patients received an initial loading dose of 600mg DUPIXENT, followed by 300mg Q2W for 16 weeks, in line with the label. Data were collected from medical records including: demographic variables, disease pattern, atopic dermatitis phenotype, location of lesions, and previous treatments. EASI score, pruritus NRS, and DLQI score were assessed at baseline and after 4 and 16 weeks of treatment.
**Percentage of pa ents, treated with DUPIXENT 300mg Q2W + TCS in LIBERTY AD CHRONOS, who reported no days of sleep disturbances. Days with sleep disturbance were assessed using item 2 on the Patient-Oriented Eczema Measure (POEM)
DUPIXENT IMPROVED MEASURES OF ANXIETY AND DEPRESSION1
18+ YEARS
Patients who were depressed or anxious at baseline achieving a clinically meaningful improvement at Week 521
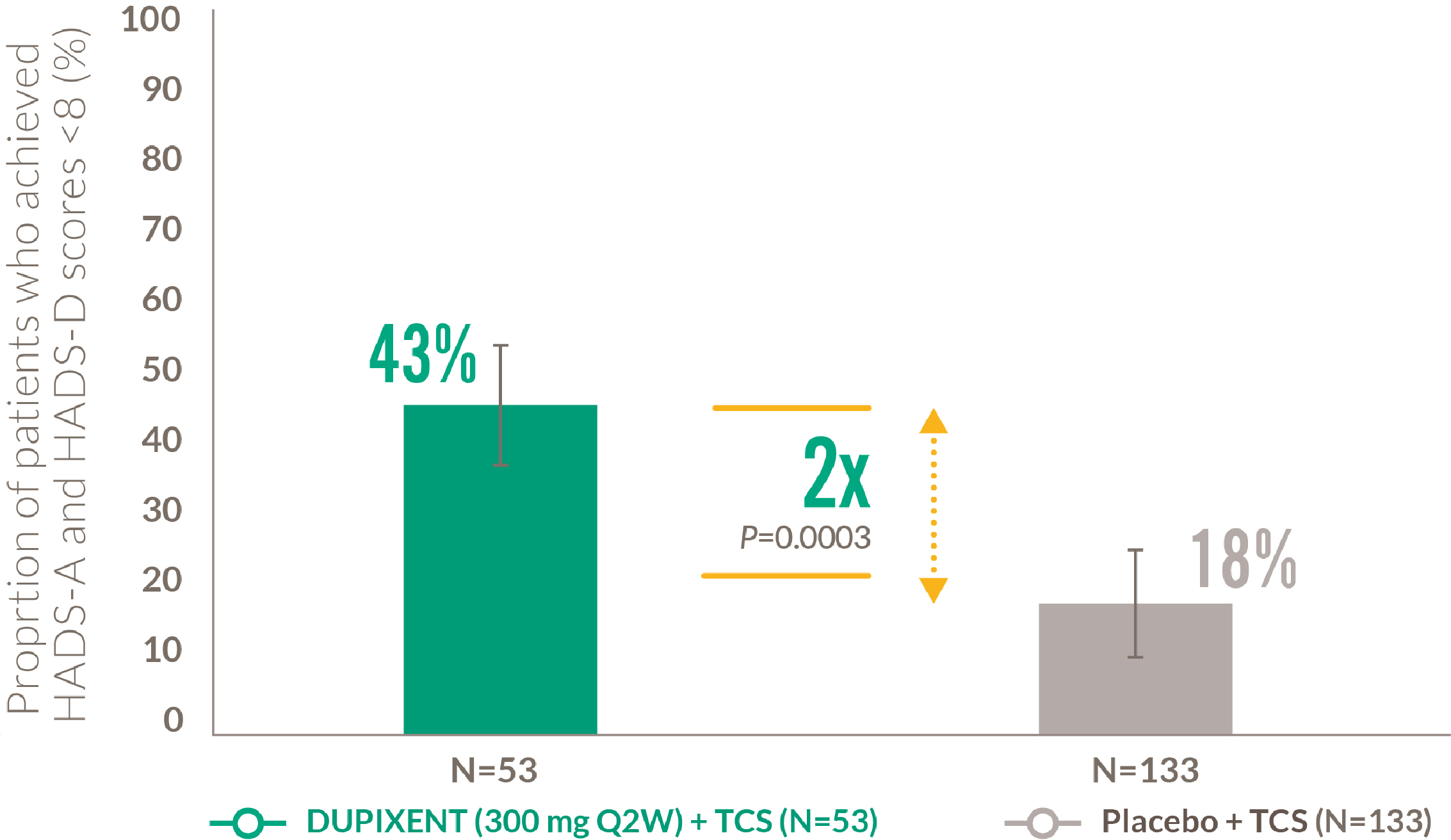
HADS-A and HADS-D scores of <8 are considered ‘normal’
At baseline in LIBERTY AD CHRONOS, 47% and 56% of patients had a HADS-A and HADS-D score ≥8, indicative of clinical symptoms of anxiety or depression, in the Placebo + TCS and DUPIXENT 300mg Q2W + TCS groups, respectively
- Blauvelt A et al. Lancet 2017; 389(10086):2287–2303.
- Data on file (AD-1224 CSR EASI). Sanofi and Regeneron Pharmaceu cals, Inc. 2022.
- Blauvelt A et al. Lancet 2017; 389(10086):2287–2303. [suppl.].
- Data on file (AD-1224 CSR DLQI). Sanofi and Regeneron Pharmaceu cals, Inc. 2022.
- Silverberg JI et al. Acta Derm Venereol 2021; 101(11):adv00585.
- Merola JF et al. J Am Acad Dermatol 2021; 84(2):495–497.
- Fargnoli MC et al. J Dermatolog Treat 2021; 32(5):507–513.
- Beck LA et al. J Eur Acad Dermatol Venereol 2021; 35(2):e130–e133.
- Barbarot S et al. J Dermatolog Treat 2022;33(1):266-277.
- Data on file (pa ent profiles SOLO) Sanofi and Regeneron Pharmaceu cals, Inc. 2022.
- Silverberg JI et al. Br J Dermatol 2019; 181:80–87.
RAPID AND SUSTAINED CONTROL AFTER THE FIRST DOSE
Rapid relief of itch and increased skin clearance, and QoL after the first dose1–4,5-13
Skin Clearance
~40% of patients achieved EASI-75 at Week 161
Itch Relief
~50% mean percentage improvement in pruritus NRS score from baseline to Week 161
Quality of Life
~60% of patients achieved a clinically meaningful improvement† in CDLQI at Week 16 3,4

≥80%
response rate‡ based on improvements in lesions, itch, or QoL1-3
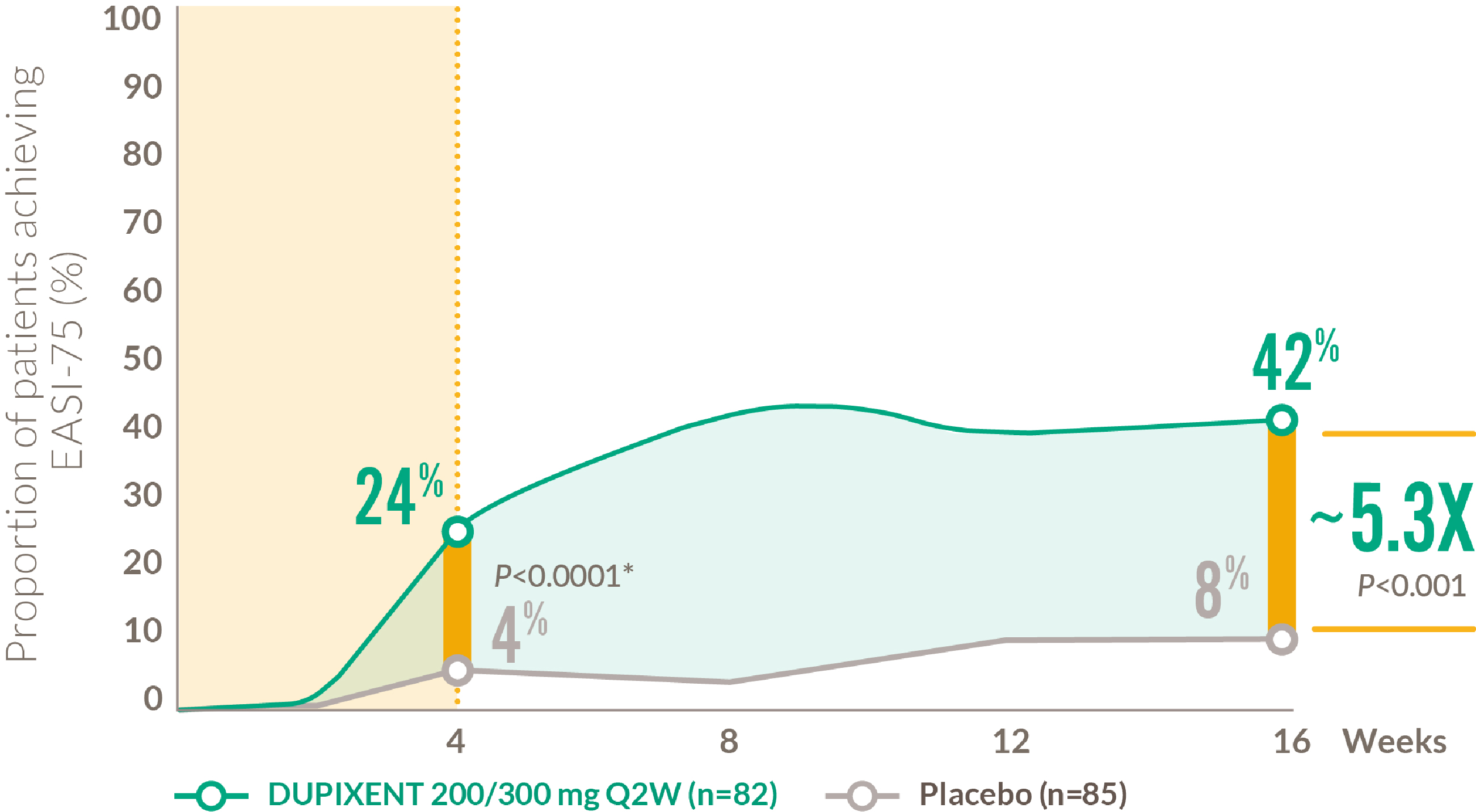
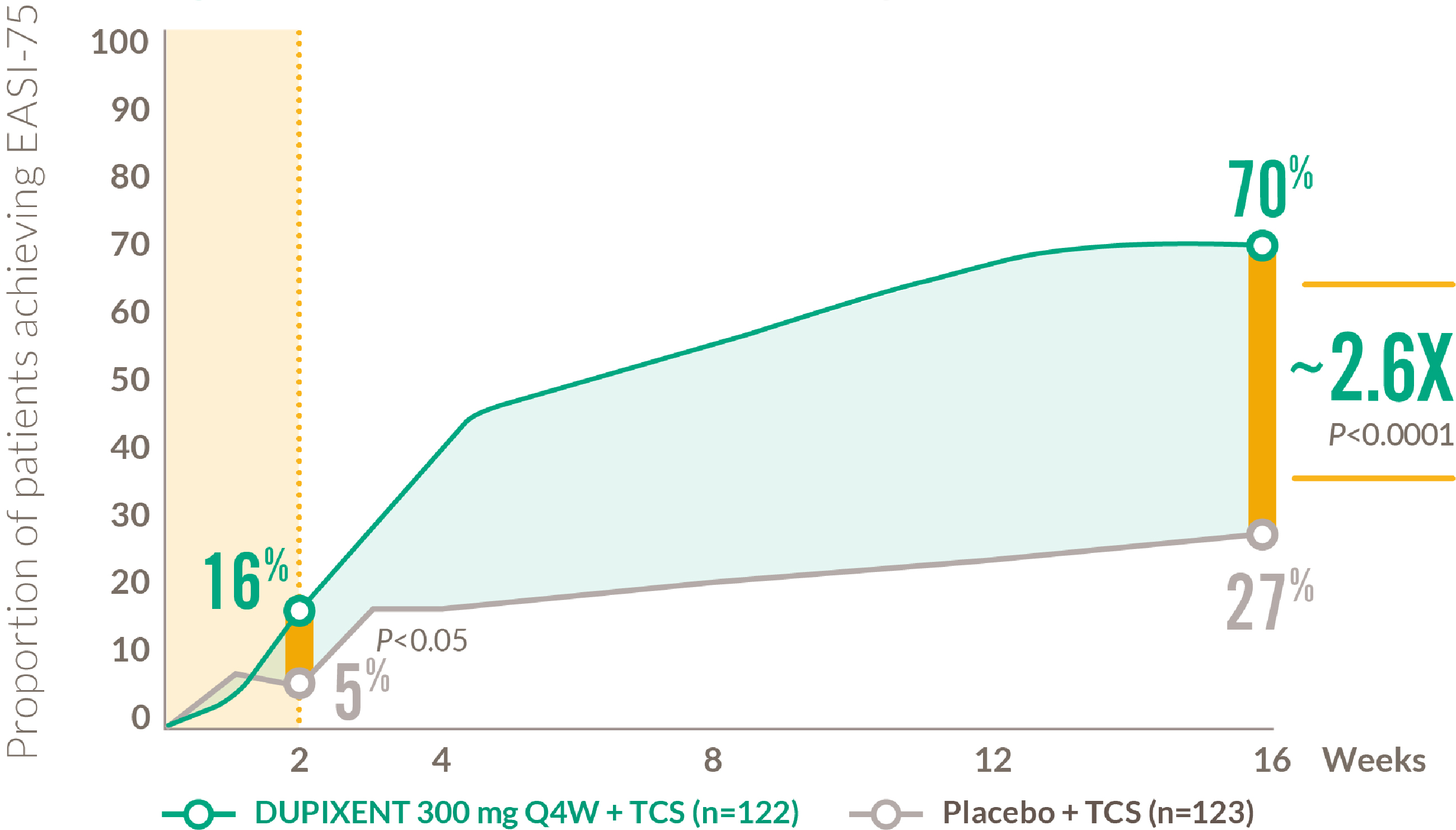
RAPID AND SUSTAINED IMPROVEMENT IN SKIN CLEARANCE AFTER THE FIRST DOSE1,2
12-17 YEARS
Proportion of patients achieving EASI-75 from baseline to Week 161,2
Coprimary endpoints in LIBERTY AD ADOL:1
- 24% of DUPIXENT patients achieved IGA 0 or 1 vs 2% of placebo patients at Week 16
- 42% of DUPIXENT patients achieved EASI-75 vs 8% of placebo patients at Week 16
*Nominal P-value
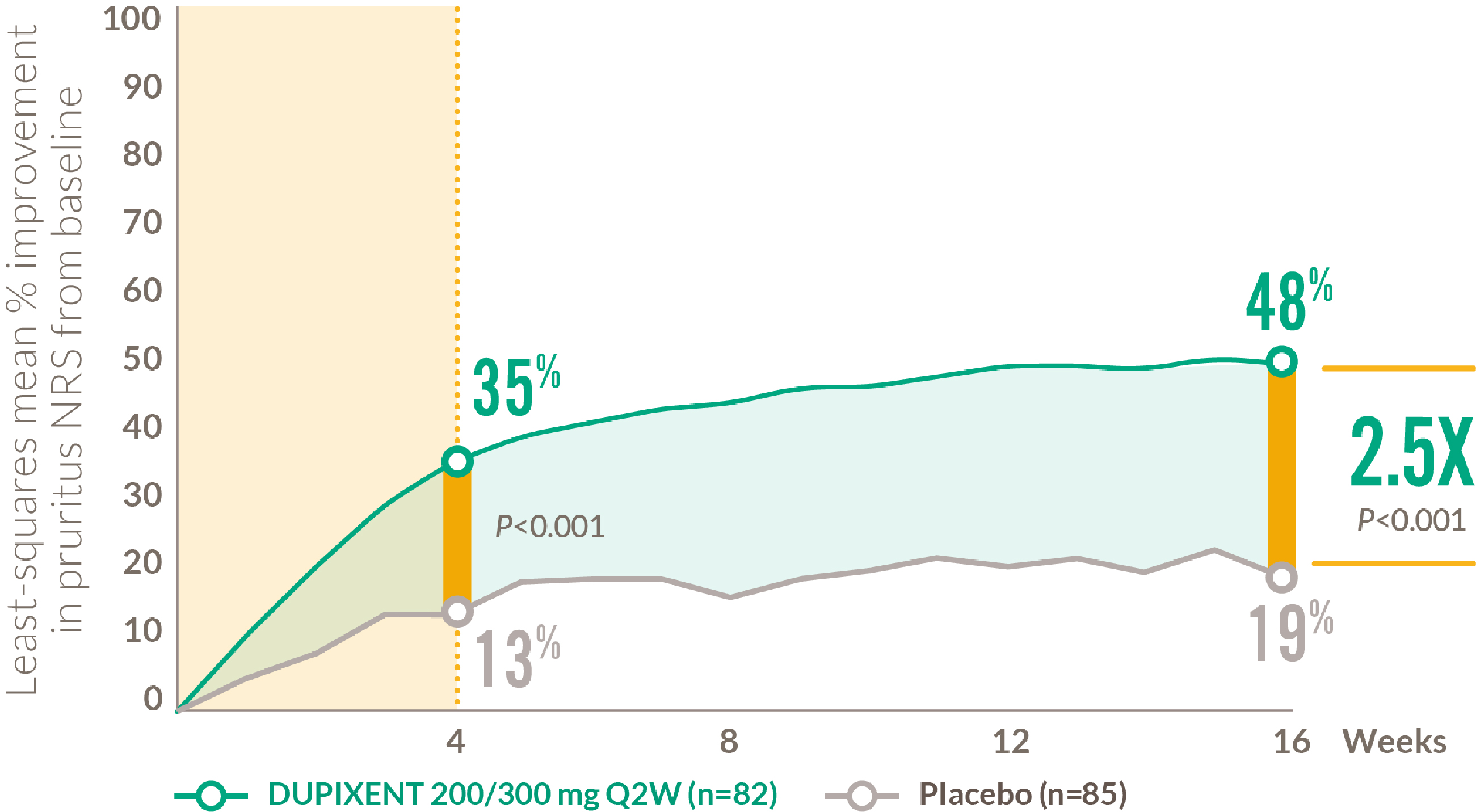
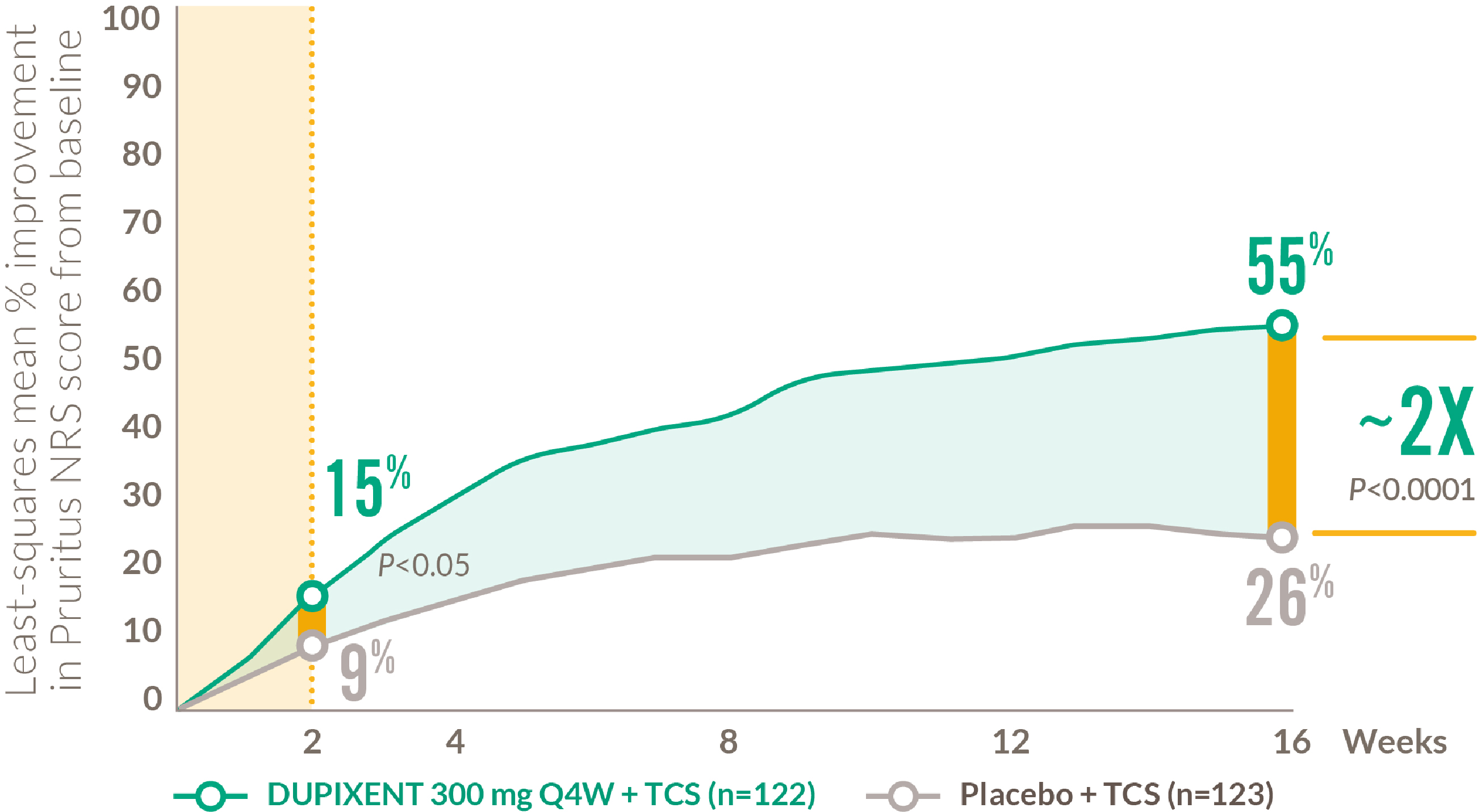
RAPID AND SUSTAINED IMPROVEMENT IN ITCH AFTER THE FIRST DOSE1
12-17 YEARS
Mean percentage improvement in pruritus NRS score from baseline to Week 161
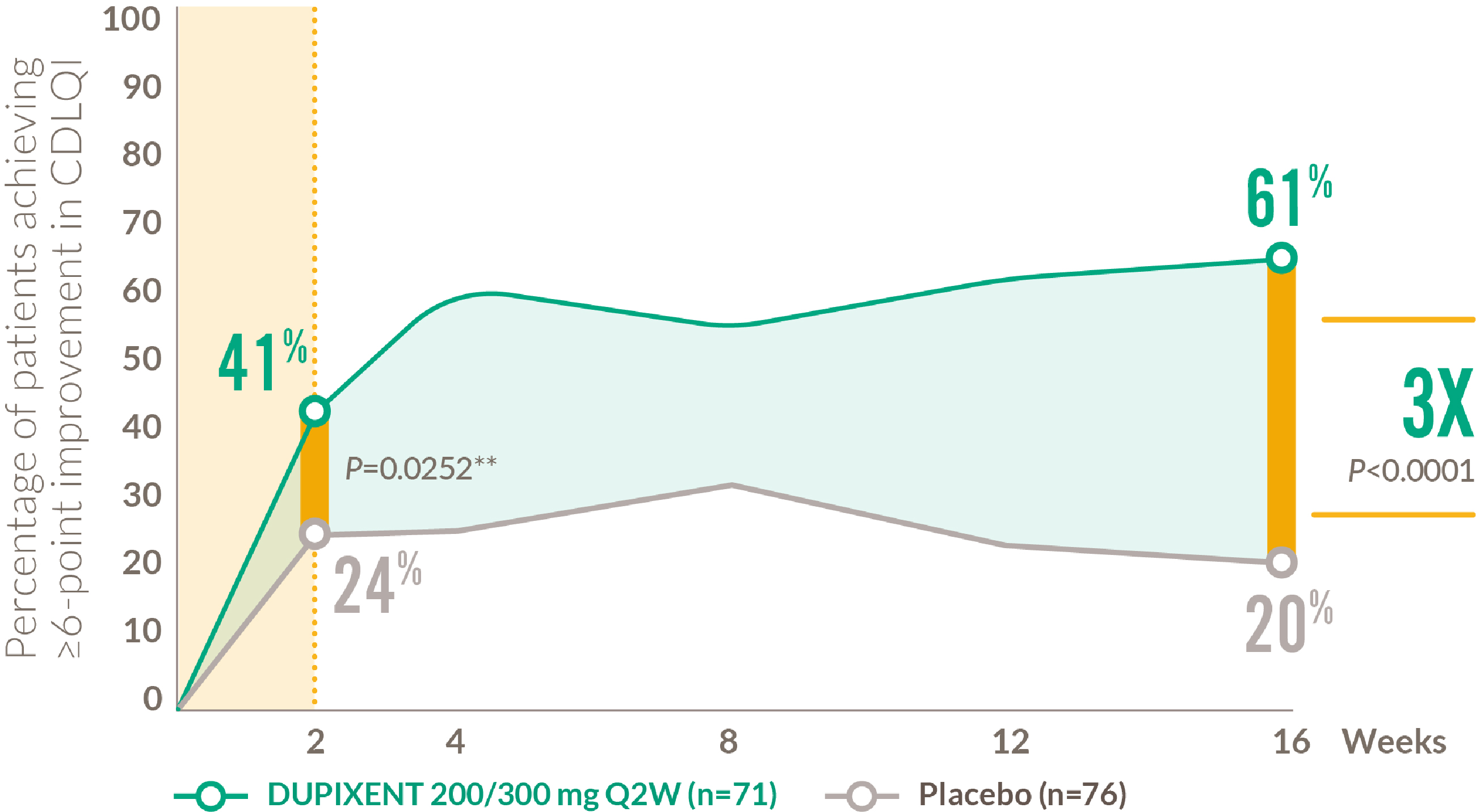
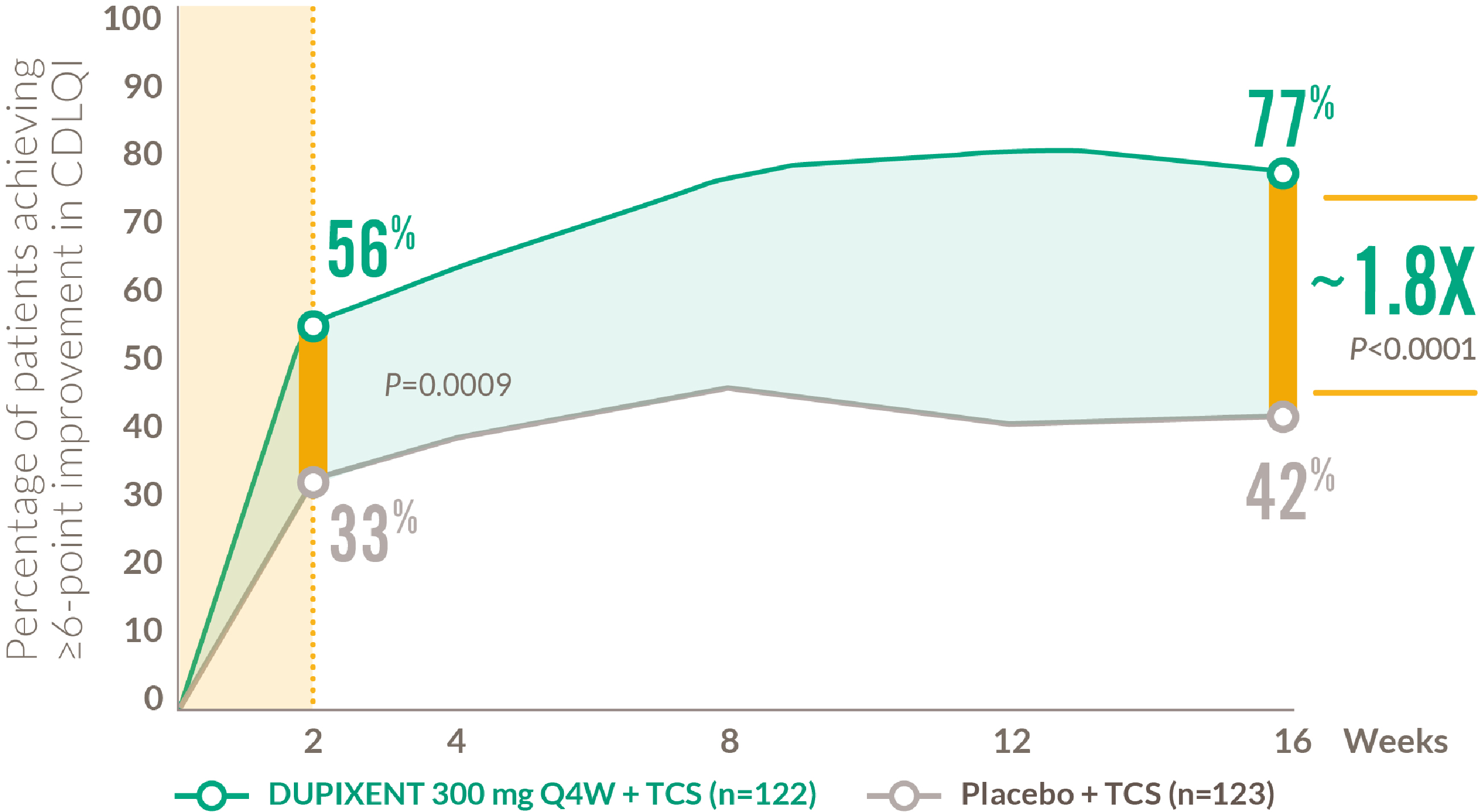
RAPID AND SUSTAINED IMPROVEMENT IN QUALITY OF LIFE AFTER THE FIRST DOSE3,4
12-17 YEARS
Patients achieving clinically meaningful improvement* in CDLQI3,4
*Defined as a ≥ 6-point improvement in CDLQI on a 0–30 point scale
**Nominal P-value
DUPIXENT REDUCED SLEEP LOSS3
12-17 YEARS
Mean improvement in SCORAD VAS sleep component from baseline to Week 163
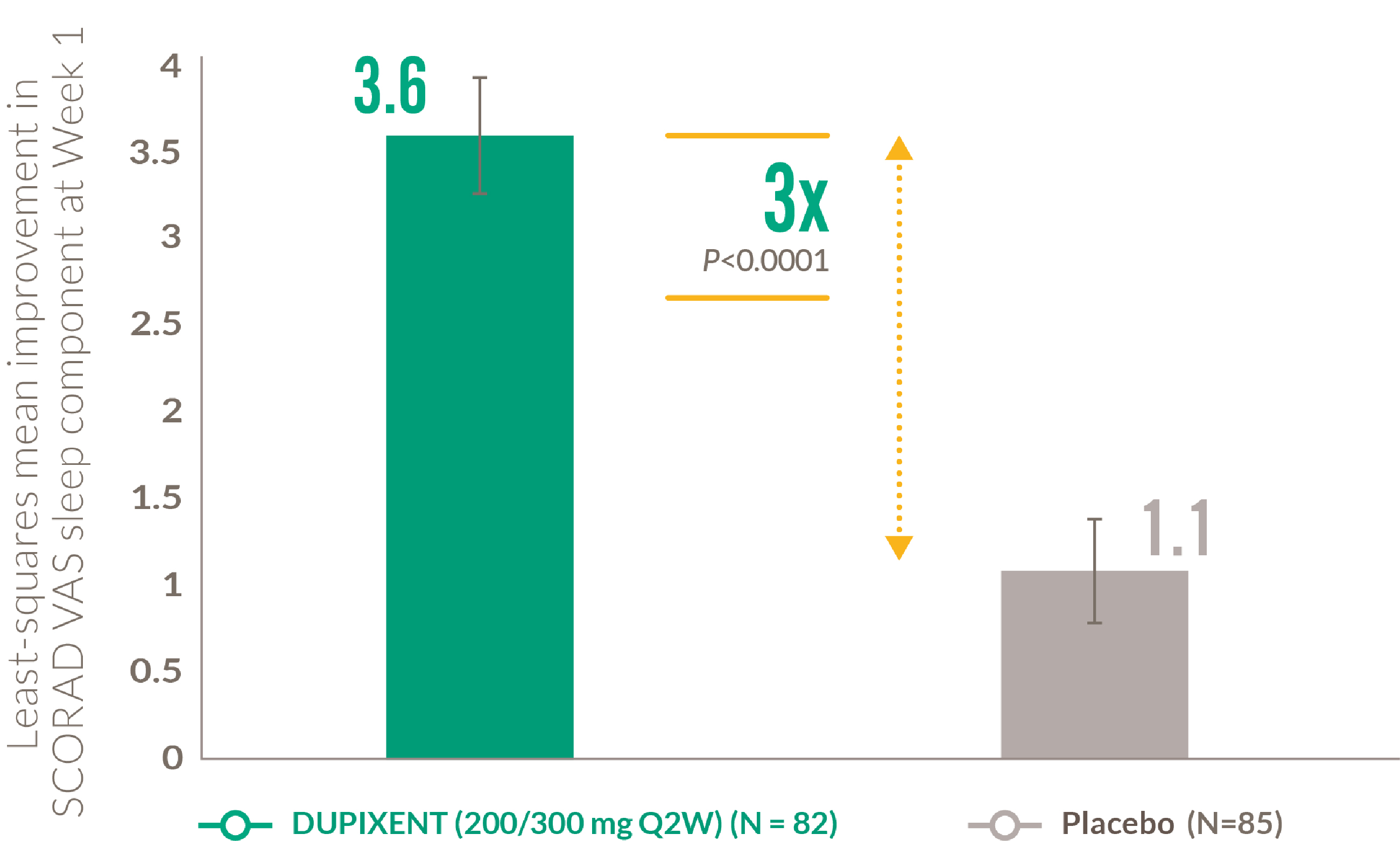
The SCORAD VAS sleep component is a scale ranging from 0 (“no sleeplessness”) to 10 (“worst imaginable sleeplessness“)
At baseline in LIBERTY AD ADOL, the mean SCORAD VAS sleep component score was 5.6 and 5.4 in the placebo and DUPIXENT 200mg/300mg Q2W groups, respectively
- Simpson EL et al. JAMA Dermatol 2020; 156(1):44–56.
- Data on file (AD-1526 EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Paller AS et al. Am J Clin Dermatol 2020; 21:119–131.
- Data on file (AD-1526 CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Blauvelt A et al. Lancet 2017; 389(10086):2287–2303.
- Blauvelt A et al. Lancet 2017; 389(10086):2287–2303. [suppl.].
- Data on file (AD-1224 CSR DLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Paller AS et al. J Am Acad Dermatol 2020; 83(5):1282–1293.
- Data on file (AD-1652 CSR CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Paller AS et al. Poster presented at the 44th Annual Meeting of the Society for Pediatric Dermatology; 2019; July 11–14; Austin, TX, USA. Poster P-16.
- Data on file (AD-1539 EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 pruritus NRS). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Paller AS et al. Presenta on at the 19th European Society for Pediatric Dermatology Annual Mee ng; 2019; May 2–4; Dubrovnik, Croa a.
- Simpson EL et al. Poster presented at the Annual Conference of the Pediatric Dermatology Research Alliance; 2019; November 14–16; Chicago, IL, USA.
RAPID AND SUSTAINED CONTROL AFTER THE FIRST DOSE
Rapid relief of itch and increased skin clearance, and QoL after the first dose1–4,5-13
Skin Clearance
~70% of patients achieved EASI-75 at Week 161
Itch Relief
~55% mean percentage improvement in pruritus NRS score from baseline to Week 161
Quality of Life
~80% of patients achieved a clinically meaningful improvement** in CDLQI at Week 164

~95%
Response rate† based on improvements in lesions, itch, or QoL5
DUPIXENT REDUCED SLEEP LOSS3
12-17 YEARS
Mean improvement in SCORAD VAS sleep component from baseline to Week 163
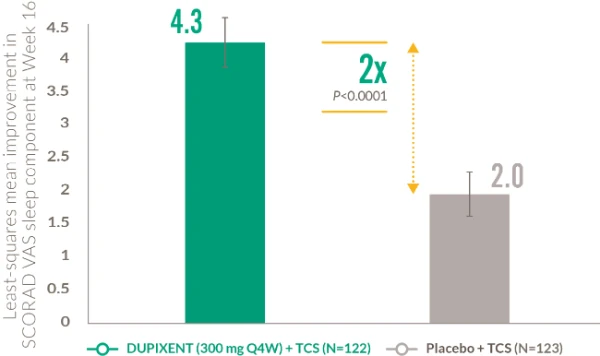
The SCORAD VAS sleep component is a scale ranging from 0 (“no sleeplessness”) to 10 (“worst imaginable sleeplessness”)
At baseline in LIBERTY AD PEDS, the mean SCORAD VAS sleep component score was 6.0 and 6.8 in the placebo and DUPIXENT 300mg Q4W +TCS groups, respectively. DUPIXENT 200mg is also available for children aged 6–11 15kg to <60kg, based on physician’s assessment.
DUPIXENT IMPROVED MEASURES OF ANXIETY AND DEPRESSION1
6-11 YEARS
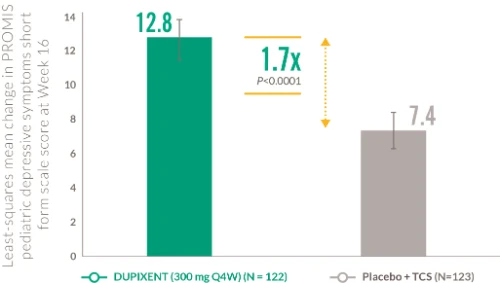
Mean change in PROMIS depressive symptoms at Week 161
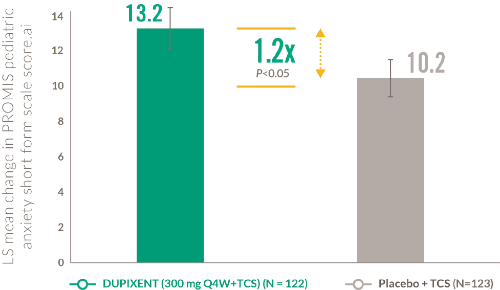
Mean change in PROMIS anxiety score at Week 161
The PROMIS pediatric depressive symptoms short form scale ranges from a score of 36.2 to 84.7, where a higher score indicates a greater severity of depressive symptoms during the past 7 days. The PROMIS pediatric anxiety short form scale ranges from a score of 34.6 to 86.4, where a higher score indicates a greater severity of anxiety during the past 7 days.
At baseline in LIBERTY AD PEDS, the mean PROMIS depressive symptoms score was 55.0 and 58.1 in the placebo + TCS and DUPIXENT 300mg Q4W + TCS groups, respectively. At baseline, the mean PROMIS anxiety score was 57.3 and 59.8 in the placebo + TCS and DUPIXENT 300mg Q4W +TCS groups, respectively. DUPIXENT 200mg is also available for children aged 6–11 15kg to <60kg, based on physician’s assessment.
- Paller A et al. J Am Acad Dermatol 2020; 83(5):1282–1293.
- Data on file (AD-1652 CSR EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1652 CSR pruritus NRS). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1652 CSR CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1652 response rate). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Shumel B and Rossi AB. The Dermatologist 2020; 28(8):42–46.
RAPID AND SUSTAINED CONTROL – CONSISTENT ACROSS ALL AGES
Rapid relief of itch and increased skin clearance, and QoL after first dose1–10
| Adult
(300mg Q2W + TCS at Week 52)1-3 |
Adolescent
(200/300mg Q2W at Week 16)6-7 |
Child
(300mg Q4W + TCS at Week 16)4-5 |
|
| Skin Clearance
Proportion of patients achieving EASI-75 |
65% | 42% | 70% |
| Itch Relief
Mean percentage improvement in pruritus NRS score from baseline |
56% | 48% | 55% |
| Quality of Life
Proportion of patients achieving a clinically meaningful improvement in quality of life measures |
80% | 61% | 77% |
Consistent improvements in itch, skin clearance, and quality of life across age groups – demonstrated in adults through to children as young as 6 years when treated with DUPIXENT compared to placebo1–10
- Blauvelt A et al. Lancet 2017; 389(10086):2287–2303.
- Blauvelt A et al. Lancet 2017; 389(10086):2287–2303. [suppl.].
- Data on file (AD-1224 CSR DLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Paller A et al. J Am Acad Dermatol 2020; 83(5):1282–1293.
- Data on file (AD-1652 CSR CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Simpson EL et al. JAMA Dermatol 2020; 156(1):44–56.
- Paller AS et al. Poster presented at the 44th Annual Mee ng of the Society for Pediatric Dermatology; 2019; July 11–14; Aus n, TX, USA. Poster P-16.
- Data on file (AD-1539 EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 pruritus NRS). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
A UNIQUE, LONG-TERM SAFETY AND TOLERABILITY PROFILE ESTABLISHED UP TO 52 WEEKS IN ADULTS1
LIBERTY AD CHRONOS
(Week 52)
| Discontinuation rates due to AEs were lower than placebo at 52 weeks1 | Comparable rates of infections reported, including serious and opportunistic2 | Lower rates of non-herpetic skin infections vs placebo+ TCS1 | ||||||
| 1.8%
DUPIXENT +TCS |
VS | 7.6%
Placebo +TCS |
0.2%
DUPIXENT +TCS |
VS | 0.6%
Placebo +TCS |
10.9%
DUPIXENT +TCS |
VS | 17.8%
Placebo +TCS |
DUPIXENT HAS A DEMONSTRATED SAFETY PROFILE UNDERPINNED BY TARGETED IMMUNOMODULATION NOT BROAD SUPPRESSION2-4
UNIQUE LONG-TERM SAFETY PROFILE
Safety and tolerability up to Week 52 in adults1
Adverse reactions for DUPIXENT in clinical studies2
| System Organ Class | Frequency | Adverse Reaction |
| Infections and infestations | Common | Conjunctivitis*
Oral herpes* |
| Blood and lymphatic system disorders | Common | Eosinophilia |
| Immune system disorders | Uncommon
Rare |
Angioedema#
Anaphylactic reaction, serum sickness reaction |
| Eye disorders | Common
Uncommon Rare |
Conjunctivitis allergic*
Keratitis*#,blepharitis*†, eye pruritus*†, dry eye*†; Ulcerative keratitis*†# |
| Skin and subcutaneous tissue disorders | Uncommon | Facial rash# |
| Musculoskeletal and connective tissue disorders | Common | Arthralgia# |
| General disorders and administration site conditions | Common | Injection site reactions (includes erythema,
oedema, pruritus, pain, and swelling) |
*Adverse event reported at SOC level of the MedDRA hierarchy. **Adverse event reported at the high-level term of the MedDRA hierarchy. †Conjunctivitis (highlevel term) includes the PTs conjunctivitis allergic, conjunctivitis bacterial, atopic keratoconjunctivitis, and conjunctivitis.‡Adjudicated.
- Blauvelt A et al. Lancet 2017; 389:2287–2303.
- DUPIXENT Summary of Product Characteristics, August 2023.
- Guttman-Yassky E et al. J Allergy Clin Immunol 2019; 143:155-172.
- Grieco T et al. Clin Dermatol 2021; 39(6):1083-1087.
ADOLESCENT SAFETY AND TOLERABILITY PROFILE CONSISTENT WITH ADULTS BASED IN 16 WEEKS DATA1,4
SAFETY PROFLE ESTABLISHED IN OVER 10,000 CLINICAL TRIAL PATIENTS SPANNING MULTIPLE AGE GROUPS ACROSS 3 INDICATIONS – ATOPIC DERMATITIS, ASTHMA, AND CHRONIC RHINOSINUSITIS WITH NASAL POLYPOSIS1,3
LIBERTY AD CHRONOS
(Week 52)
| No discontinuations due to AEs with DUPIXENT1 | No serious AEs reported with DUPIXENT1 | Lower rates of non-herpetic skin infections vs placebo1 | ||||||
| 0%
DUPIXENT |
VS | 1.2%
Placebo |
0%
DUPIXENT |
VS | 1.2%
Placebo |
9.8%
DUPIXENT |
VS | 18.8%
Placebo |
DUPIXENT HAS A DEMONSTRATED SAFETY PROFILE UNDERPINNED BY TARGETED IMMUNOMODULATION NOT BROAD SUPPRESSION2-4
UNIQUE LONG-TERM SAFETY PROFILE
Safety and tolerability up to Week 16 in adolescents in LIBERTY AD ADOL1
AEs in ≥5% of patients during the 16-week treatment period in LIBERTY AD ADOL1
| Adverse event, n (%) | DUPIXENT 200 0r 300mg Q2W (n=82) | Placebo (n=85) |
| Skin infection (adjudicated) | 9 (11.0) | 17 (20.0) |
| Upper respiratory tract infection | 10 (12.2) | 15 (17.6) |
| Headache | 9 (11.0) | 9 (10.6) |
| Conjunctivitis* | 8 (9.8) | 4 (4.7) |
| Nasopharyngitis | 3 (3.7) | 4 (4.7) |
| Infections and infestations (SOC) | 34 (41.5) | 37 (43.5) |
| Injection site reactions | 7 (8.5) | 3 (3.5) |
| Herpes viral infections | 1 (1.2) | 3 (3.5) |
*Includes the atopic keratoconjunctivitis, conjunctivitis, conjunctivitis allergic, conjunctivitis bacterial, conjunctivitis viral.
- Simpson EL et al. JAMA Dermatol 2020; 156(1):44–56.
- DUPIXENT Summary of Product Characteristics. August 2023.
- Guttman-Yassky E et al. J Allergy Clin Immunol 2019; 143:155-172.
- Grieco T et al. Clin Dermatol 2021; 39(6):1083-1087.
A UNIQUE SAFETY AND TOLERABILITY PROFILE ESTABLISHED UP TO WEEK 16 IN CHILDREN AS YOUNG AS 6 YEARS OLD1,3
SAFETY PROFLE ESTABLISHED IN OVER 10,000 CLINICAL TRIAL PATIENTS SPANNING MULTIPLE AGE GROUPS ACROSS 3 INDICATIONS – ATOPIC DERMATITIS, ASTHMA, AND CHRONIC RHINOSINUSITIS WITH NASAL POLYPOSIS1,4
LIBERTY AD CHRONOS
(Week 52)
| No discontinuations due to AEs with DUPIXENT2 | Comparable rate of serious AEs between DUPIXENT + TCS and placebo + TCS2 | Lower rates of skin infections vs placebo + TCS2 | ||||||
| 0%
DUPIXENT +TCS |
VS | 1.7%
Placebo +TCS |
1.7%
DUPIXENT +TCS |
VS | 1.7%
Placebo +TCS |
5.8%
DUPIXENT +TCS |
VS | 13.3%
Placebo +TCS |
DUPIXENT HAS A DEMONSTRATED SAFETY PROFILE UNDERPINNED BY TARGETED IMMUNOMODULATION NOT BROAD SUPPRESSION1,4,5
UNIQUE SAFETY PROFILE
Safety and tolerability up to Week 16 in children 6–11 years in LIBERTY AD PEDS2
AES IN >5% OF PATIENTS DURING THE 16 WEEK TREATMENT PERIOD IN LIBERTY AD PEDS1
| Adverse event, n (%) | DUPIXENT 300mg Q4W + TCS (n=120) | Placebo (n=120) |
| Nasopharyngitis | 15 (12.5) | 8 (6.7) |
| Upper respiratory tract infection | 13 (10.8) | 12 (10.0) |
| Vomiting | 6 (5.0) | 8 (6.7) |
| Headache | 6 (5.0) | 10 (8.3) |
| Conjunctivitis* | 8 (6.7) | 5 (4.2) |
| Skin infection (adjudicated)** | 7 (5.8) | 16 (13.3) |
| Injection site reactions | 7 (8.5) | 3 (3.5) |
| Injection site reactions† | 12 (10.0) | 7 (5.8) |
If a systemic hypersensitivity reaction (immediate or delayed) occurs, DUPIXENT should be discontinued immediately and appropriate therapy initiated1
DUPIXENT 200mg Q2W is also available for children aged 6–11 15kg to <60kg, based on physician’s assessment. *Conjunctivitis cluster (narrow conjunctivitis) includes preferred terms conjunctivitis, conjunc tivitis allergic, conjunctivitis bacterial, conjunctivitis viral, and atopic keratoconjunctivitis. **Skin infec ons were adjudicated on a case-by-case basis and included bacterial, viral, and fungal infections. †Adverse event reported at the high-level term of the MedDRA hierarchy.
- DUPIXENT Summary of Product Characteristics. August 2023.
- Paller AS et al. J Am Acad Dermatol 2020; 83:1282–1293.
- Data on File (AD 1434 Compliance). Sanofi and Regeneron Pharmaceuticals, Inc. 2019.
- Guttman-Yassky E et al. J Allergy Clin Immunol 2019; 143:155-172.
- Grieco T et al. Clin Dermatol 2021; 39(6):1083-1087.
A UNIQUE SAFETY AND TOLERABILITY PROFILE DEMONSTRATED IN PATIENTS AS YOUNG AS 6 YEARS OLD1-3
Only atopic dermatitis therapy approved in patients as young as 6 years1
DUPIXENT has a unique safety profile underpinned by targeted immunomodulation and not broad immunosuppression1-3
 Not metabolized through the liver or excreted through the kidneys2 Not metabolized through the liver or excreted through the kidneys2 |

No requirement for initial lab testing or ongoing lab monitoring5 |

No known drug-drug interactions2 |
| Adult
(Week 52)6 |
Adolescent
(Week 16)7 |
Child
(Week 16)8 |
|||||||
| No or lower rate of discontinuations due to AEs vs placebo | 1.8%
DUPIXENT +TCS |
VS | 7.6%
Placebo +TCS |
0.0%
DUPIXENT |
VS | 1.2%
Placebo |
0.0%
DUPIXENT +TCS |
VS | 1.7%
Placebo +TCS |
| Comporable rate of serious AEs vs placebo | 3.6%
DUPIXENT +TCS |
VS | 5.1%
Placebo +TCS |
0.0%
DUPIXENT |
VS | 1.2%
Placebo |
1.7%
DUPIXENT +TCS |
VS | 1.7%
Placebo +TCS |
| Lowe rates of non-herpetic skin infections vs placebo | 10.9%
DUPIXENT +TCS |
VS | 17.8%
Placebo +TCS |
9.8%
DUPIXENT |
VS | 18.8%
Placebo |
5.8%
DUPIXENT +TCS |
VS | 13.3%
Placebo +TCS |
The safety profile of DUPIXENT is consistent across ages groups – from children aged 6 years through to adults6-9
- DUPIXENT Summary of Product Characteristics. August 2023.
- Guttman-Yassky E et al. J Allergy Clin Immunol 2019; 143:155-172.
- Grieco T et al. Clin Dermatol 2021; 39(6):1083-1087.
- Wollenberg A et al. Br J Dermatol 2020;182(5):1120–1135.
- Blauvelt A et al. Lancet 2017; 389:2287–2303.
- Simpson EL et al. JAMA Dermatol 2020; 156(1):44–56.
- Paller AS, et al. J Am Acad Dermatol. 2020; 83(5):1282–1293.
- Data on file (AD-1526 adverse events). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
CONSISTENT RESULTS SEEN THROUGH 4 YEARS OF REAL-WORLD EXPERIENCE
| Location | Skin clearance (EASI) | Itch (pruritus) | Qualityof life (DLQI) |
| Japan
(N=153)1 |
85%
Mean percent change from baseline to Week 80 |
58%
Mean percentage change from baseline to week 80 |
74%
Mean percentage change from baseline to week 80 |
| USA and Canada
(N=563)2 |
82%
Mean improvement from baseline to Month 18 |
61%
Mean improvement from baseline to Month 18 |
77%
Mean improvement from baseline to Month 18 |
| Italy
(N=165)3 |
89%
Mean improvement from baseline to Week 52 |
84%
Mean improvement from baseline to Week 52 |
90%
Mean improvement from baseline to Week 52 |
| The Netherlands
(N=218)4 |
85%
Mean percent change from baseline to Week 52 |
71%
Mean percent change from baseline to Week 52 |
83%
Mean percent change from baseline to Week 52 |
| The UK
(N=156)3 |
91%
Median improvement from baseline to Week 26–30 |
N/A | 91%
Median improvement from baseline to Week 26–30 |
| Germany
(N=56)3 |
79%
Mean improvement from baseline to Week 24 |
56%
Mean improvement from baseline to Week 24 |
66%
Mean improvement from baseline to Week 24 |
| Spain
(N=70)7 |
77%
Mean improvement from baseline to Week 24 |
N/A | 63%
Mean improvement from baseline to Week 24 |
| Austria
(N=94)8 |
78%
Mean improvement from baseline to Week 24 |
N/A | 71%
Mean improvement from baseline to Week 24 |
| South Korea
(N=99)9 |
88%
Mean percent change from baseline to Week 52 |
66%
Mean percent change from baseline to Week 52 |
69%
Mean percent change from baseline to Week 52 |
| France
(N=241)10 |
77%
Mean percent change from baseline to Week 12 |
N/A | 69%
Mean percent change from baseline to Week 12 |
- de Wijs LEM et al. Br J Dermatol 2021; 185(3):555–562.
- Bagel J et al. Poster presented at the 30th Congress of the European Academy of Dermatology and Venereology; 2021; September 29–October 2; Virtual Meeting. Poster P0257.
- Napolitano M et al. Dermatol Ther (Heidelb) 2021; 11:355–361.
- Ariëns LFM et al. Acta Derm Venereol. 2021;101(10):adv00573.
- Kreeshan FC et al. Dermatol Ther (Heidelb) 2021; 11:149–160.
- Abraham S et al. Br J Dermatol 2020; 183:382-384.
- Armario-Hita JC et al. Br J Dermatol 2019; 181:1072–1074.
- Quint T et al. J Clin Med 2020; 9(4):1241.
- Jang DH et al. Sci Rep. 2021;11(1):23539.
- Faiz S et al. J Am Acad Dermatol 2019; 81(1):143–151.
FAVORABLE TOLERABILITY PROFILE ACROSS REAL-WORLD STUDIES
TOLERABILITY PROFILE IN REAL-WORLD STUDIES
| Low discontinuation rates across studies1-4 | |||
|
2%
|
2%
|
2%
|
2%
|
RANDOMIZED CONTROL TRIAL
LIBERTY AD CHRONOS
Discontinuation rate6*
2%
At 52 weeks
| No lab monitoring required3-5 | ||
 |
 |
 |
| No lab monitoring required3-5 | ||

0% |
1% |
7% |
LIBERTY AD CHRONOS
Injection site reactions6*6*
15%
ONLY ATOPIC DERMATITIS THERAPY WITH 4 YEARS SAFETY DATA7
- Napolitano M et al. Dermatol Ther (Heidelb) 2021; 11:355–361.
- Quint T et al. J Clin Med 2020; 9(4):1241.
- Kreeshan FC et al. Dermatol Ther (Heidelb) 2021; 11:149–160.
- de Wijs LEM et al. Br J Dermatol 2020; 182(2):418–426.
- Uchida H et al. J Am Acad Dermatol 2021; 84(2):547–550.
- Blauvelt A et al. Lancet 2017; 389:2287–2303.
- Beck L et al. Am J Clin Dermatol 2022; 23(3):393–408.
REAL-WORLD STUDIES OF DUPIXENT DEMONSTRATE GREATER LEVELS OF PERSISTENCE THAN THAT SEEN IN THE CHRONOS PIVOTAL TRIAL1–5
PERSISTENCE IN REAL-WORLD STUDIES

97%**
|
88%**
At 204 weeks (95/109)1 |

91%†
|
88%†
At 104 weeks (104/109)1 |

94%‡
|
|

82%§
|
|
|
87%¶
|
RANDOMIZED CONTROL TRIAL
LIBERTY AD CHRONOS*
86%
At 52 weeks (77/90)
At 2 years real-world evidence demonstrates >80% persistence2,6
Real-world studies of DUPIXENT demonstrate greater levels of persistence at 52 weeks than clinical trials1-5
- Hong M and Silverberg JI. Poster presented at the virtual Revolutionizing Atopic Dermatitis (RAD) Conference; 2020; April 5; Chicago IL, USA.
- Spekhorst LS et al. Allergy 2020; 75(9):2376–2379.
- Pereyra-Rodriquez JJ et al. Br J Dermatol 2021; 184(1): 175–176.
- Dal Bello G et al. Dematol Ther 2020; 33(6):e13979.
- Igawa K et al. Poster presented at the 30th Congress of the European Academy of Dermatology and Venereology; 2021; September 29–October 2; Virtual
- Meeting. Poster P0272. 6. de Wijs LEM et al. Br J Dermatol 2020; 182(2):418–426
- Blauvelt A et al. Lancet 2017; 389:2287–2303.
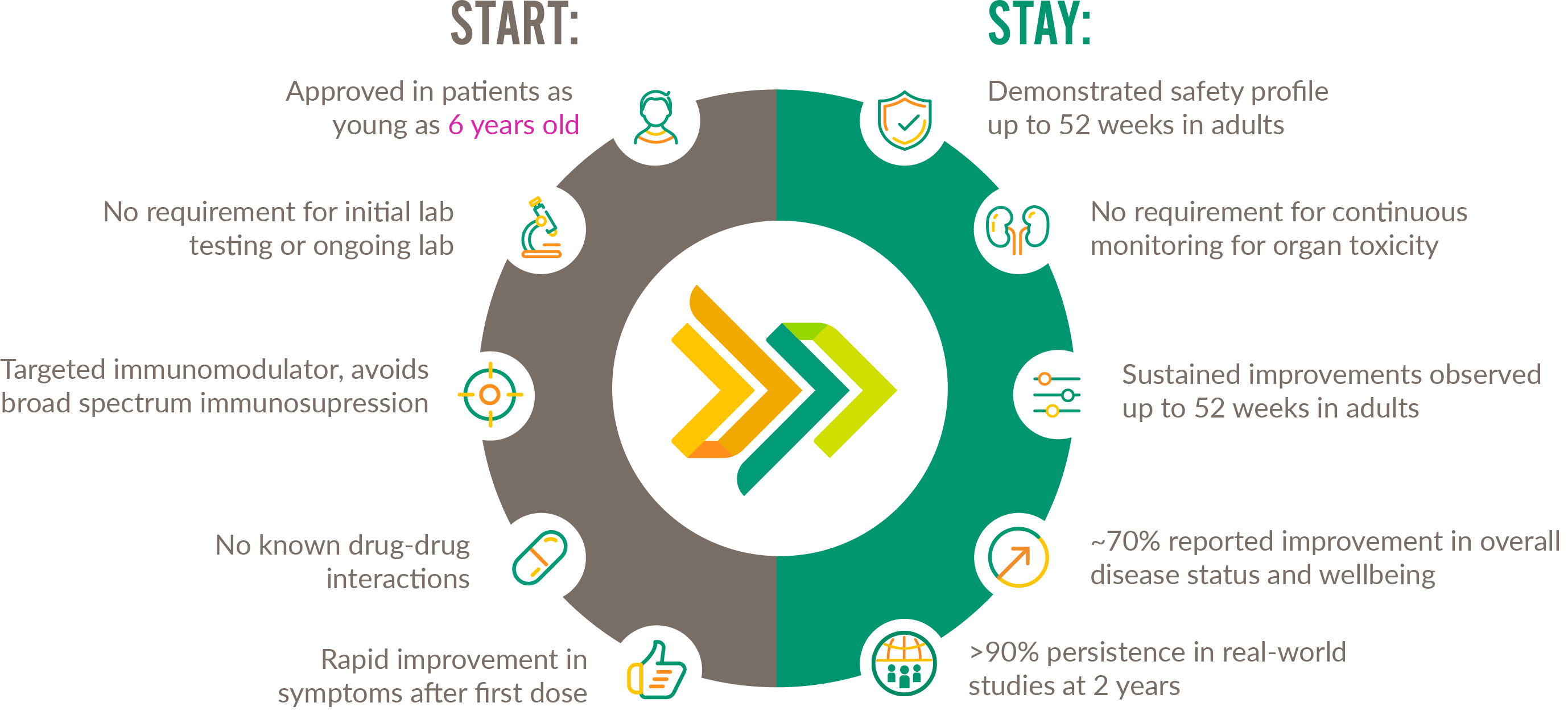
START WITH EASE, STAY WITH CONFIDENCE
From initiation to follow-up, DUPIXENT makes it easy for ALL AGE GROUPS to achieve lasting relief1-20
85% PATIENT SATISFACTION WITH DUPIXENT TREATMENT AT 1 YEAR21
DUPIXENT HAS HIGH LEVELS OF PATIENT SATISFACTION21,22
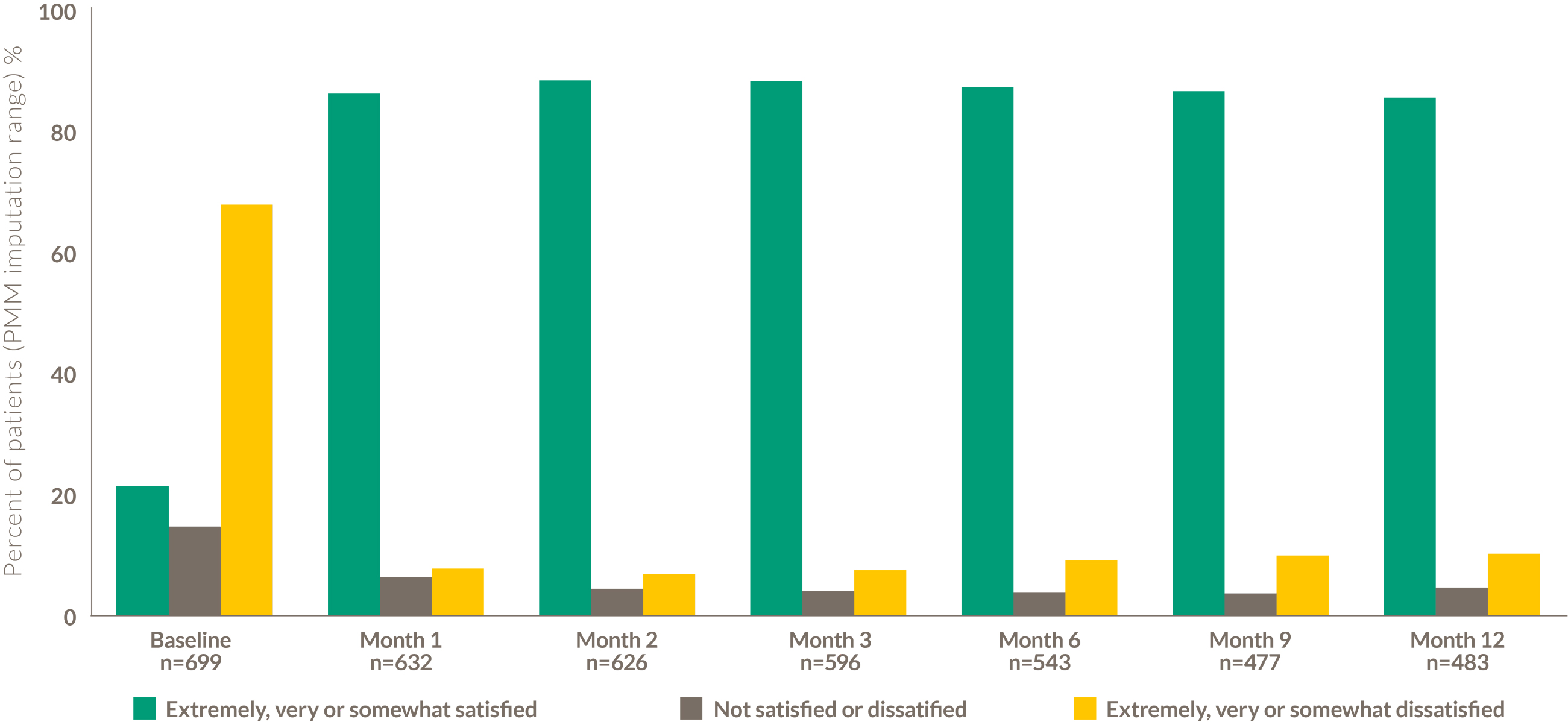
85%
OF ADULT PATIENTS TREATED WITH DUPIXENT WERE VERY/EXTREMELY/ SOMEWHAT SATISFIED AT 12 MONTHS VS 18% BEFORE STARTING
AFTER INITIATING DUPIXENT, THE PROPORTION OF PATIENTS WHO WERE EXTREMELY SATISFIED INCREASED AT EACH FOLLOW-UP
Prospective, longitudinal patient survey of adult patients who had not been treated with DUPIXENT prior to this study (N=699). A sensitivity analysis, pattern mixture modelling (PMM) was conducted for imputation of missing values.
- DUPIXENT Summary of Product Characteristics. August 2023.
- Wollenberg A et al. Br J Dermatol 2020;182(5):1120-1135.
- Blauvelt A et al. Lancet 2017; 389:2287–2303. [suppl.].
- Data on file (AD-1224 CSR EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1224 CSR DLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1652 CSR EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1652 CSR pruritus NRS). Sanofi and Regeneron Pharmaceticals, Inc. 2022.
- Data on file (AD-1652 CSR CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 pruritus NRS). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1526 EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1526 pruritus NRS). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1526 CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Beck L et al. Am J Clin Dermatol 2022; 1–16. doi: 10.1007/s40257-022-00685-0.
- Blauvelt A et al. Lancet 2017; 389:2287–2303.
- Blauvelt A et al. Poster presented at the Revolutionizing Atopic Dermatitis Conference; 2021; June 13; Virtual Conference. Poster 469.
- Cork MJ et al. Presented at the 2021 Revolutionizing Atopic Dermatitis (RAD) Conference; Virtual Conference; June 13, 2021.
- Simpson EL et al. Poster presented at the 30th Congress of the European Academy of Dermatology and Venereology; 2021; September 29–October 2; Virtual Meeting. Poster P0723.
- Kojanova M et al. J Dermatolog Treat. 2022. doi: 10.1080/09546634.2022.2043545.
- Strober B et al. JAMA Dermatol 2022; 158(2):142–150.
- Strober B et al. JAMA Dermatol. 2022;158(2):142–150. [suppl.]
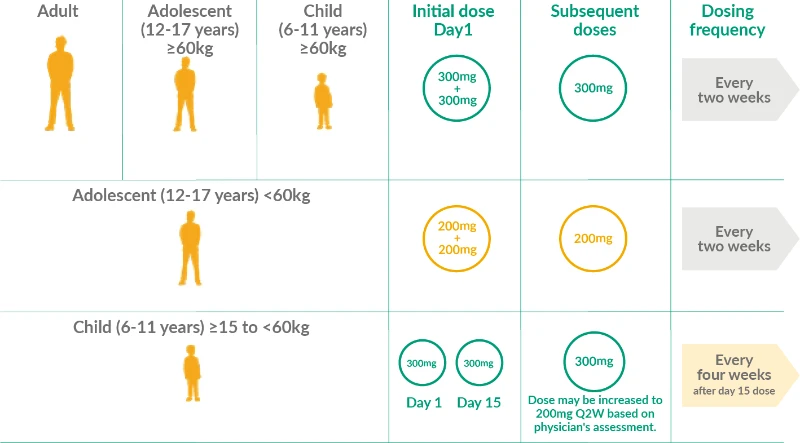
DUPIXENT GIVES YOUR PATIENTS CONVENIENT ADMINISTRATION OPTIONS
DUPIXENT offers biweekly dosing for adults, adolescents, and children who weigh 60kg or more, and dosing once every four weeks for children ≥15 to <60kg1
DUPIXENT now provides you and your patients with a pre-filled syringe1
DUPIXENT gives your patients the choice of at-home or in-office administration1
- DUPIXENT Summary of Product Characteristics. August 2023.

RAPID AND SUSTAINED CONTROL – CONSISTENT ACROSS ALL AGES
Sustained improvement of itch, skin clearance, and quality of life up to 52 weeks, with rapid control after first dose1-16
UNIQUE LONG-TERM SAFETY PROFILE
Only atopic dermatitis therapy
Approved in patients as young as 6 years1
START WITH EASE, STAY WITH CONFIDENCE
DUPIXENT is not an immunosuppressant1
85% patient satisfaction with DUPIXENT treatment at 1 year in adults17*
~340,000 ATOPIC DERMATITIS PATIENTS TREATED WITH DUPIXENT WORLDWIDE18
*In adult patients with atopic dermatitis
- DUPIXENT Summary of Product Characteristics. August 2023.
- Blauvelt A et al. Lancet 2017; 389:2287–2303.
- Data on file (AD-1224 CSR). Sanofi and Regeneron Pharmaceuticals, Inc. 2016.
- Blauvelt A et al. Lancet 2017; 389:2287–2303. [suppl.].
- Data on file (AD-1224 CSR DLQI rate). Sanofi and Regeneron Pharmaceuticals, Inc. 2021.
- Data on file (AD-1652 CSR EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2019.
- Data on file (AD-1652 CSR CDLQI rate). Sanofi and Regeneron Pharmaceuticals, Inc. 2019.
- Paller AS et al. J Am Acad Dermatol 2020; 83(5):1282–1293.
- Cork MJ et al. Poster presented at the Revolutionizing Atopic Dermatitis Conference; 2021; June 13; Virtual Conference. Poster 468.
- Data on file (AD-1652 CSR pruritus NRS). Sanofi and Regeneron Pharmaceuticals, Inc. 2019.
- Simpson EL et al. JAMA Dermatol 2020; 156(1):44–56.
- Data on file (AD-1526 CSR EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2019.
- Paller AS et al. Am J Clin Dermatol 2020; 21:119–131.
- Data on file (AD-1539 EASI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 pruritus NRS). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Data on file (AD-1539 CDLQI). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
- Strober B et al. JAMA Dermatol 2022;158(2):142–150.
- Data on file (Patient numbers, May 2022). Sanofi and Regeneron Pharmaceuticals, Inc. 2022.
MAT-BH-2400435/V1/August 2024