

Sanofi is a trusted player in cardiovascular care, with a reputation for providing well established antihypertensive care solutions. Over the last three decades, millions of patients have been treated with Sanofi antihypertensive medications.1

Potent BP reduction2-5

Effects beyond blood pressure reduction for irbesartan and amlodipine 2,6,7
- • Renal protection, with proven benefits in hypertensive diabetic patients with nephropathy8-10
- • Coronary protection due to Systolic and Diastolic blood pressure reduction shown in I-ADD and I-COMBINE studies3,4
- Sanofi Periodic Benefit Risk Evaluation Report 2019.Data
- Aprovasc. Summary of Product Characteristics. Saudi Arabia. 2015.
- Bobrie G. I-COMBINE study: assessment of efficacy and safety profile of irbesartan/amlodipine fixed-dose combination therapy compared with amlodipine monotherapy in hypertensive patients uncontrolled with amlodipine 5 mg monotherapy: a multicenter, phase III, prospective, randomized, open-label with blinded-end point evaluation study. Clin Ther. 2012; 34 (8): 1705-19.
- Bobrie G. I-ADD study: assessment of efficacy and safety profile of irbesartan/amlodipine fixed-dose combination therapy compared with irbesartan monotherapy in hypertensive patients uncontrolled with irbesartan 150 mg monotherapy: a multicenter, phase III, prospective, randomized, open-label with blinded-end point evaluation study. Clin Ther. 2012; 34 (8): 1720-34 e3.
- Ishimitsu T, et al. The therapeutic advantage of combination antihypertensive drug therapy using amlodipine and irbesartan in hypertensive patients:Analysis of the post-marketing survey data from PARTNER (Practical combination therapy of Amlodin and angiotensin II Receptor blocker; safety and efficacy in patients with hypertension) study. Clin Exp Hypertens. 2015; 37 (7): 542-50.
- Amlodipine. Summary of product characteristics. UK, 2018.
- Aprovel. Summary of product characteristics. UK, 2018.
- Parving HH, et al. The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med. 2001; 345 (12): 870-8.
- Ravera M, et al. Prevention and treatment of diabetic nephropathy: the program for irbesartan mortality and morbidity evaluation. J Am Soc Nephrol. 2005;16 Suppl 1: S48-52.
- Lewis EJ, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001; 345 (12): 851-60.

APROVASC® is an appropriate choice for single-pill combination antihypertensives.1
- Individual agents offer CV and/or renal protection beyond blood pressure lowering alone.1,2,3
- Because single-pill combinations offer greater patient convenience.4,5
- With good tolerability profiles.1
- And a full range of dosing possibilities.1

150 mg/5 mg film-coated tablets

150 mg/10 mg film-coated tablets

300 mg/5 mg film-coated tablets

300 mg/10 mg film-coated tablets
The balanced and convenient approach to trusted and potent blood pressure reduction.6,7,8
- Aprovasc. Summary of Product Characteristics. Saudi Arabia. 2015.
- Amlodipine. Summary of Product Characteristics. UK,2018.
- Aprovel. Summary of Product Characteristics. UK,2018.
- DiPette DJ, et al. Fixed-dose combination pharmacologic therapy to improve hypertension control worldwide: Clinical perspective and policy implications. J Clin Hypertens. 2019;21(1): 4-15.
- Sica DA. Rationale for fixed-dose combinations in the treatment of hypertension: the cycle repeats. Drugs. 2002; 62 (3): 443-62.
- Sanofi Periodic Benefit Risk Evaluation Report. 2019. Data on file.
- Bobrie G. I-ADD study: assessment of efficacy and safety profile of irbesartan/amlodipine fixed-dose combination therapy compared with irbesartan monotherapy in hypertensive patients uncontrolled with irbesartan 150 mg monotherapy: a multicenter, phase III, prospective, randomized, open-label with blinded-end point evaluation study. Clin Ther. 2012; 34 (8): 1720-34 e3.
- Bobrie G. I-COMBINE study: assessment of efficacy and safety profile of irbesartan/amlodipine fixed-dose combination therapy compared with amlodipine monotherapy in hypertensive patients uncontrolled with amlodipine 5 mg monotherapy: a multicenter, phase III, prospective, randomized, open-label with blinded-end point evaluation study. Clin Ther. 2012; 34 (8): 1705-19.
UNMET NEEDS
Hypertension is the leading cause of disability and mortality in KSA amongst CVDs1
- Hypertension is increasing in prevalence 50 in KSA affecting more than one fourth of the adult Saudi population2
- Recent report about cardiovascular risk factors among the Saudi population presented a prevalence of 31.4% for hypertension.3
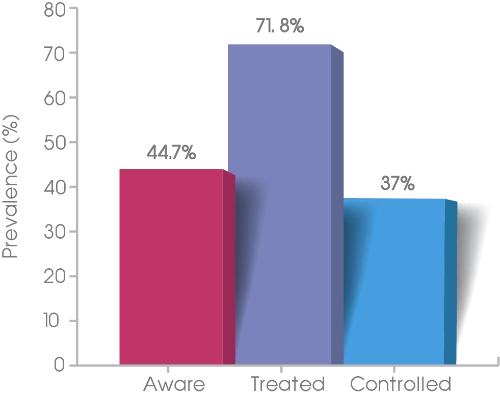
- Less than half of the hypertensives were aware of their disease in this survey in KSA.4
A cross-sectional study aimed at estimating prevalence, awareness, treatment, control, and predictors of hypertension among Saudi adult population. Multistage stratified sampling was used to select 4758 adult participants. Three blood pressure measurements using an automatic sphygmomanometer, sociodemographic, and antihypertensive modalities were obtained. The overall prevalence of hypertension was 25.5%.
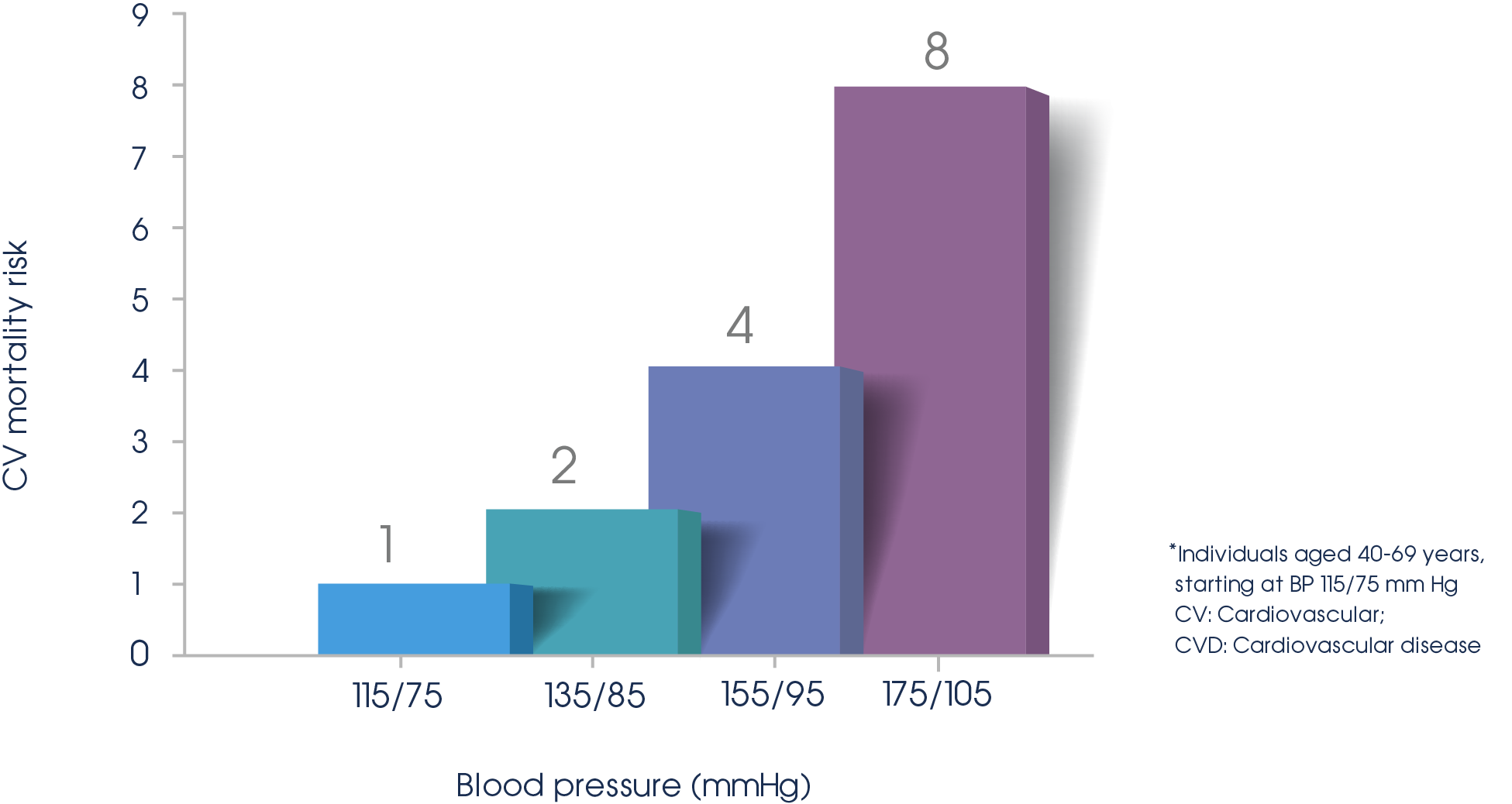
Each 10/20 mmHg increase, doubles the risk of CVD*6
CV mortality risk by blood pressure
Reductions in blood pressure of 10 mmHg are associated with up to 40% reductions in CV risk.7
Meta-analysis of 61 prospective, observational studies involving 1 million adults with no previous vascular disease during 12.7 million person-years.1
10 mmHg decrease in mean SBP

reduction in
IHD mortality7

reduction in risk of
stroke mortality7
CV: Cardiovascular; DBP: Diastolic blood pressure; IHD: Ischaemic heart disease; SBP: Systolic blood pressure.
- World Health Organization (WHO). The Investment Case for Non communicable Disease Prevention and Control in the Kingdom of Saudi Arabia. Available at: https://www.undp.org/content/dam/saudi_arabia/docs/Publications/180326%20MOH%20 KSA%20NCDs%202017.pdf. Last accessed: March,2020.
- Al-Nozha MM, Abdullah M, Arafah MR, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28(1):77-84.
- Aldiab A, Shubair MM, Al-Zahrani JM, et al. Prevalence of hypertension and prehypertension and its associated cardioembolic risk factors; a population based crosssectional study in Alkharj, Saudi Arabia. BMC Public Health. 2018;18(1):1327.
- Saeed AA, Al-Hamdan NA, Bahnassy AA, Abdalla AM, Abbas MA, Abuzaid LZ. Prevalence, Awareness, Treatment, and Control of Hypertension among Saudi Adult Population: A National Survey. Int J Hypertens. 2011; 2011:174135.
- Li YT, Wang HH, Liu KQ, et al. Medication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care Settings: A Cross-Sectional Analysis. Medicine (Baltimore). 2016;95(20):e3572.
- Chobanian AV, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood pressure. JNC 7 report. JAMA. 2003. 289 (19):2560-72
- Lewington S, et al. Age-specific relevance of usual blood pressure to vascular mortality: a metaanalysis of individual data for one million adults in 61 prospective studies. Lancet. 2002; 360 (9349): 1903-13.
COMBINATION THERAPY
At least 75% of patients require combination therapy to achieve contemporary blood pressure targets.1

European Society of Cardiology / European Society of Hypertension (ESC/ESH)
European guidelines recommend Initiation of antihypertensive therapy with a two-drug combination.2
It is recommended to initiate an antihypertensive treatment with a two-drug combination, preferably in a single-pill combination.2*
* The exceptions are frail older patients and those at low risk and with grade 1 hypertension (particularly if SBP is <150 mmHg).
Office blood pressure thresholds for treatment by age category2
| 18 - 65 YEARS | ≥140 | ≥140 | ≥140 | ≥140 |
| 65 -79 YEARS | ≥140 | ≥140 | ≥140 | ≥140 |
| ≥80 YEARS | ≥160 | ≥160 | ≥160 | ≥160 |
| Office DBP treatment target range (mmHg) | ≥90 | ≥90 | ≥90 | ≥90 |
a. Treatment may be considered in these very high-risk patients with high–normal SBP (i.e. SBP 130–140 mmHg). CAD: coronary artery disease; CKD: chronic kidney disease (includes diabetic and non-diabetic CKD); DBP: diastolic blood pressure;SBP: systolic blood pressure; TIA: transient ischaemic attack.

American College of Heart Association (ACC/AHA)
Clinical Practice Guideline: Executive Summery
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ ASPC/NMA/PCNA/ Guideline for the Prevention, detection, Evaluation, and Management of High Blood Pressure in Adults: Excecutive Summary
A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
At least 75% of patients require combination therapy to achieve contemporary blood pressure targets1
RECOMMENDATIONS:
- • BP goals for patients with hypertension: For adults with confirmed hypertension and known CVD or 10-year ASCVD event risk of 10% or higher, a BP target of less than 3 80/130 mmHg is recommended.3
- • Choice of initial monotherapy versus initial combination therapy Initiation of antihypertensive drug therapy with 2 first-line agents of different classes, either as separate agents or in a fixed-dose combination, is recommended in adults with stage 2 hypertension and an average BP more than 10/20 mmHg above their BP target.3
ASCVD atherosclerotic cardiovascular disease; BP: blood pressure; CVD: cardiovascular disease.4
- Gradman AH, et al. Combination therapy in hypertension. J Am Soc Hypertens. 2010; 2 (2): 90-8. 9.
- Williams B, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018; 39 (33): 3021-104.
- Whelton PK, et al. 2017 ACC/AHA/AAPA/ABC/ ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018; 71 (19): e127-e248
DRUG ADHERENCE
Non-adherence to medication is one of the key factors in Poor blood pressure control.1
Approximately 1 out of 2 patients don’t adhere to prescribed medications1
Average adherence even for newly treated patients remains below 30%2
And over 40% do not achieve blood pressure control3
NEW CONCEPTS TO IMPROVE PATIENT ADHERENCE.4
Detecting poor adherence to drug therapy4
-
Emphasize treatment adherence as one of the major causes of poor BP control
A single-pill combination treatment strategy could improve BP control4
- The initial preferred treatment for most patients is the two-drug combination therapy
- Simplified treatment algorithms with:
- Preferred use of an ACE-inhibitor or an ARB combined with a CCB
- And/or a thiazide/thiazide-like diuretic, as the core treatment strategy for most patients
- With beta-blockers used for specific indications
SINGLE-PILL COMBINATIONS IMPROVE ADHERENCE.5
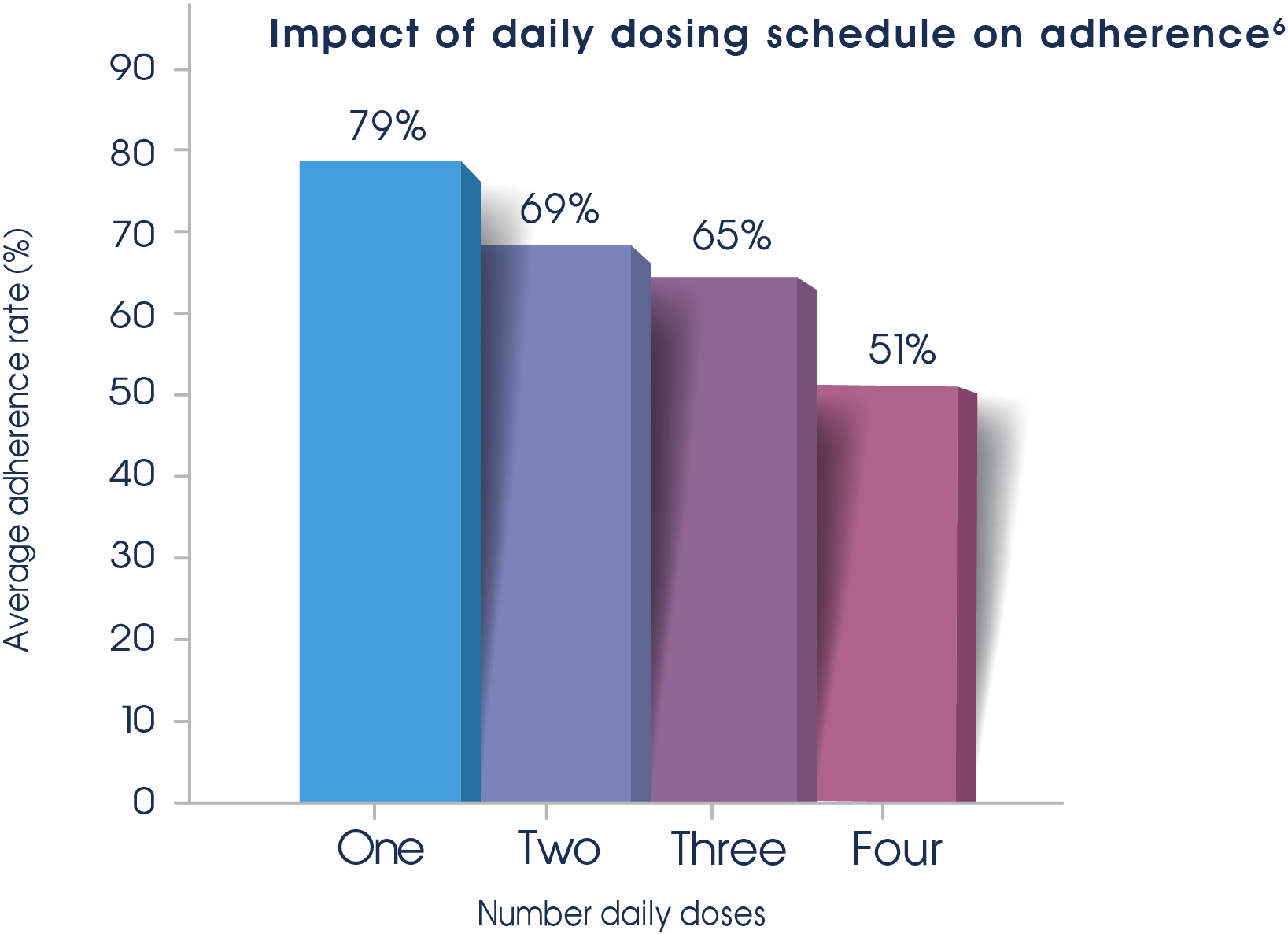
Meta-analysis 76 studies involving electronic monitoring of medication compliance between 1986 and 2000.6
For older adults, single-pill combination antihypertensive therapy is associated with a significantly lower risk of composite clinical outcomes.1
PATIENTS ARE MORE LIKELY TO PERSIST WITH ARBS THAN WITH OTHER ANTIHYPERTENSIVES.7
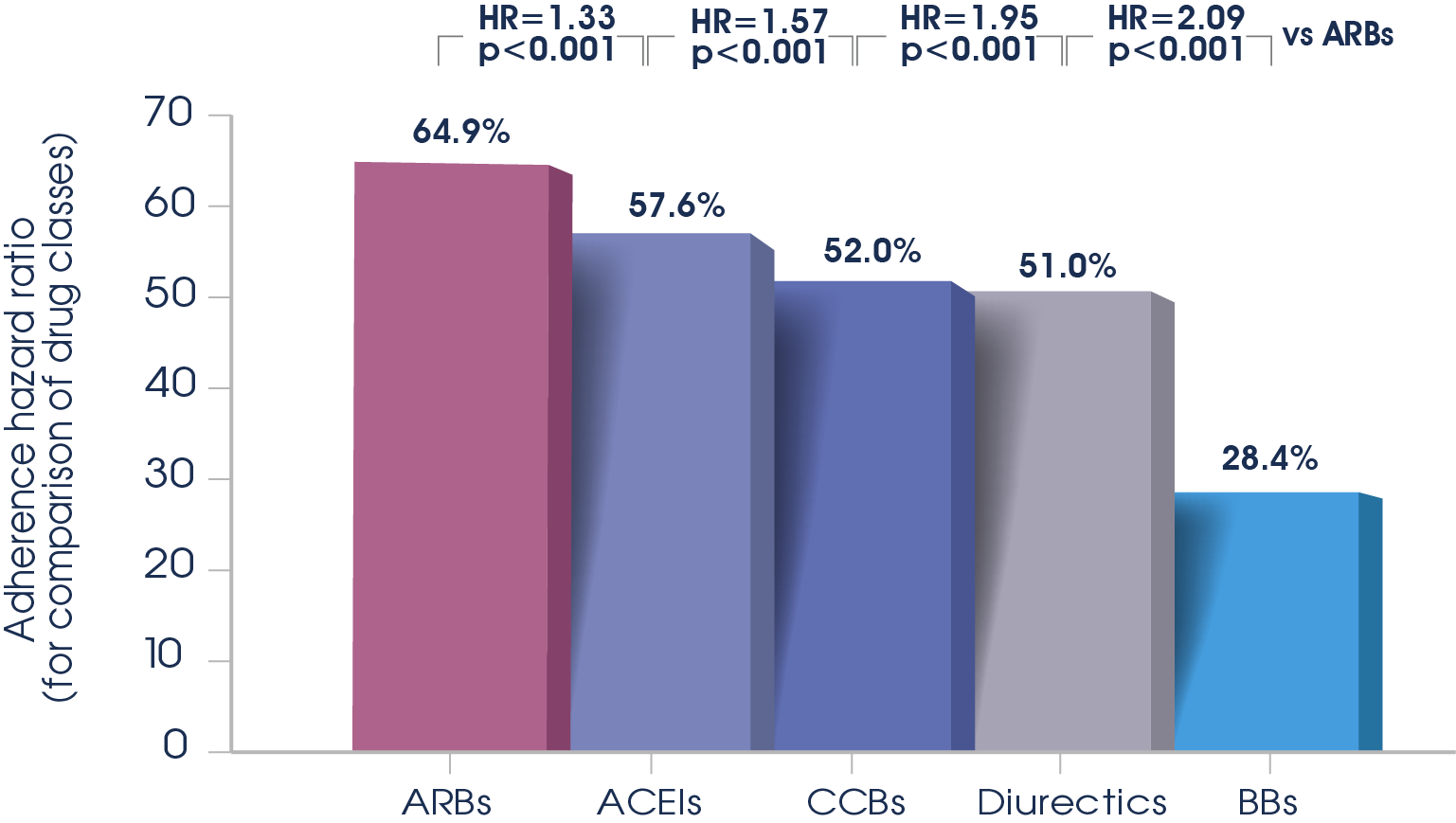
Meta-analysis of 17 studies that measured adherence to antihypertensives using medication refill data that could be used to calculate a measure of relative risk of adherence7
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; BB: beta blocker; CCB: calcium channel blocker; HR: hazard ratio.
Single-pill combinations have been shown to improve adherence and extending time on medication by 28% 8†
†28% more days covered with single-pill combinations versus multi-pill combinations in a cohort of 13,350 hypertensive individuals 66 years and older8

- Krousel-Wood M, et al. Medication adherence: a key factor in achieving blood pressure control and good clinical outcomes in hypertensive patients. Curr Opin Cardiol. 2004; 19 (4): 357-62.
- Mancia G, Two-drug combinations as first-step antihypertensive treatment. Circ Res. 2019; 124 (7): 1113-23.
- Bakris G, et al. Review of blood pressure control rates and outcomes. J Am Soc Hypertens. 2014; 8 (2): 127-41.
- Williams B, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018; 39 (33): 3021-104.
- Verma AA, et al. Fixed-dose combination antihypertensive medications, adherence, and clinical outcomes: A population-based retrospective cohort study. PLoS Med. 2018; 15 (6): e1002584.
- Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001; 23 (8): 1296-310.
- Kronish IM, et al. Meta-analysis: impact of drug class on adherence to antihypertensives. Circulation. 2011; 123 (15): 1611-21.
- Verma AA, et al. Fixed-dose combination antihypertensive medications, adherence, and clinical outcomes: A population-based retrospective cohort study. PLoS Med. 2018; 15 (6): e1002584.
APROVASC® EFFICACY

Providing potent blood pressure reduction, renal and coronary protection, and the ultimate simplicity of a single-pill combination, in a full range of doses to accommodate individual patients needs.1-6
is more potent than amlodipine alone3
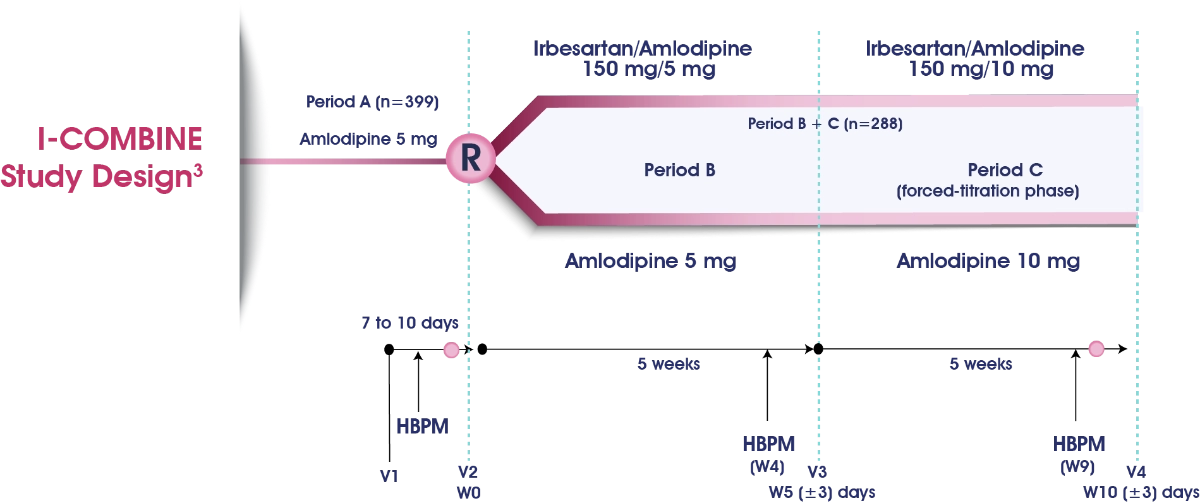
Trial Objective: To determine whether the antihypertensive efficacy of the fixed-dose combination irbesartan 150 mg/Amlodipine 5 mg (I150/A5) was superior to that of amlodipine 5 mg (A5) monotherapy in lowering home systolic blood pressure (HSBP) after 5 weeks’ treatment.
Conclusion: Data from this adult population with essential hypertension suggest greater efficacy with the fixed-dose combination I150/A5 over A5 monotherapy in lowering SBP after 5 weeks. Both treatment regimens were well tolerated throughout the study.
HBPM, home blood pressure measurement; W, week; V, visit.
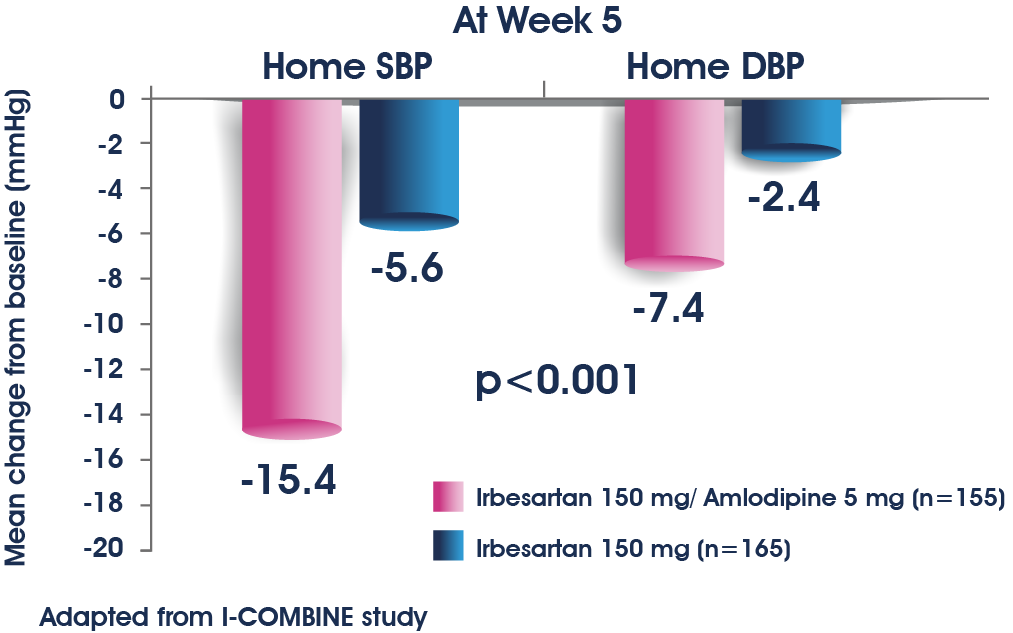
Mean change from baseline in home systolic (SBP)† and diastolic (DBP) blood pressure
†Mean change in home SBP from baseline to Week 5 is the primary endpoint. Intention-to-treat population.4
Blood pressure (BP) values at week 10 and mean changes from baseline: intention-to-treat population3
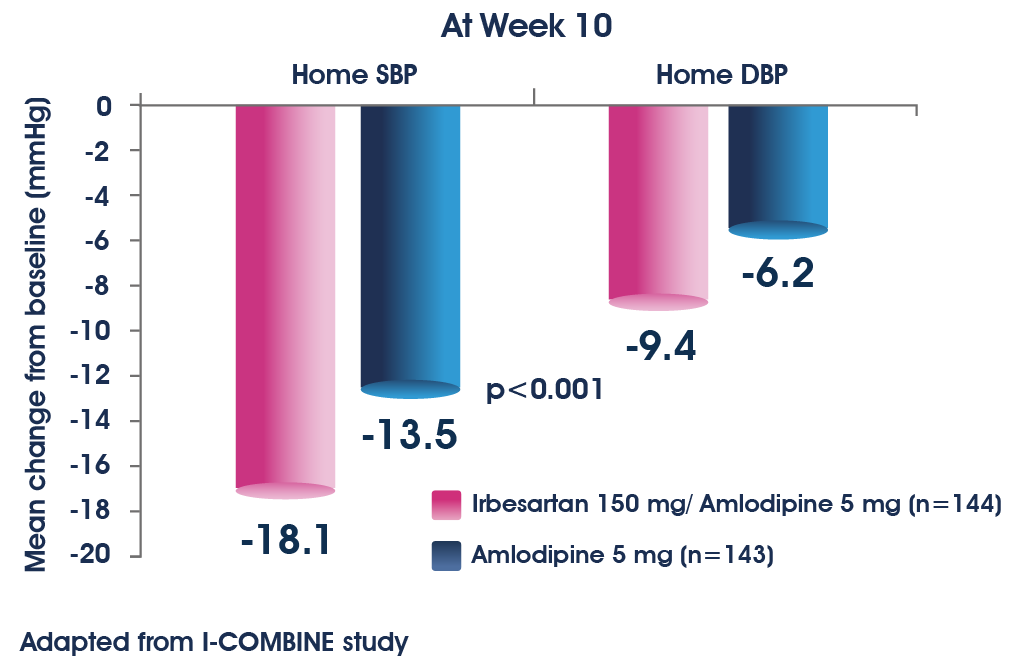
Compared with baseline, APROVASC®achieved a significantly greater reduction in mean home SBP than Amlodipine monotherapy at both weeks 5 and 104
significantly decreases the office BP in hypertensive patients.5
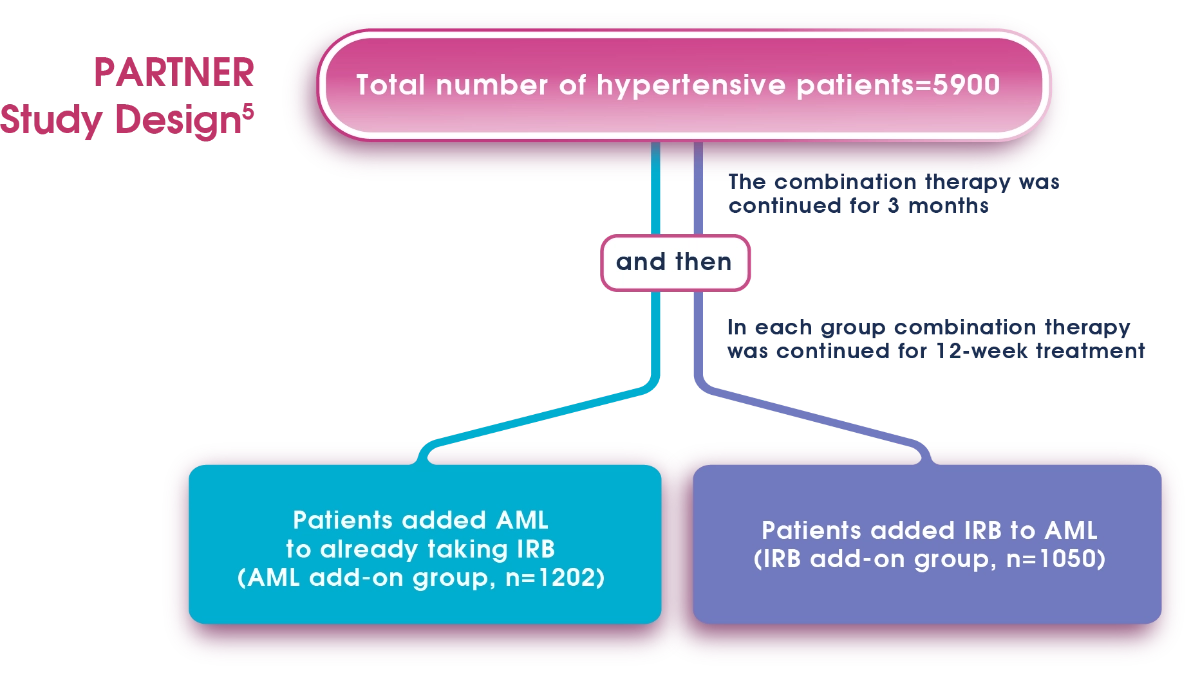
These two groups were extracted to examine the efficacy and safety of AML and IRB combination.
Trial Objective: To examine the therapeutic advantage of combination of antihypertensive drug therapy using amlodipine and irbesartan in hypertensive patients.
Conclusion: The combination therapy with AML and IRB swiftly and certainly lowers BP with a small chance of causing adverse effects. In addition, this combination is advantageous in lowering serum uric acid and is suitable for protecting kidney in CKD patients. Tablet containing AML and IRB seems promising in maintaining high adherence and exhibiting the benefits of this combination therapy efficiently.
AML, Amlodipine; IRB, Irbesartan.
Time-course changes of blood pressure in the Amlodipine (AML) add-on group and the Irbesartan (IRB) add-on group.5
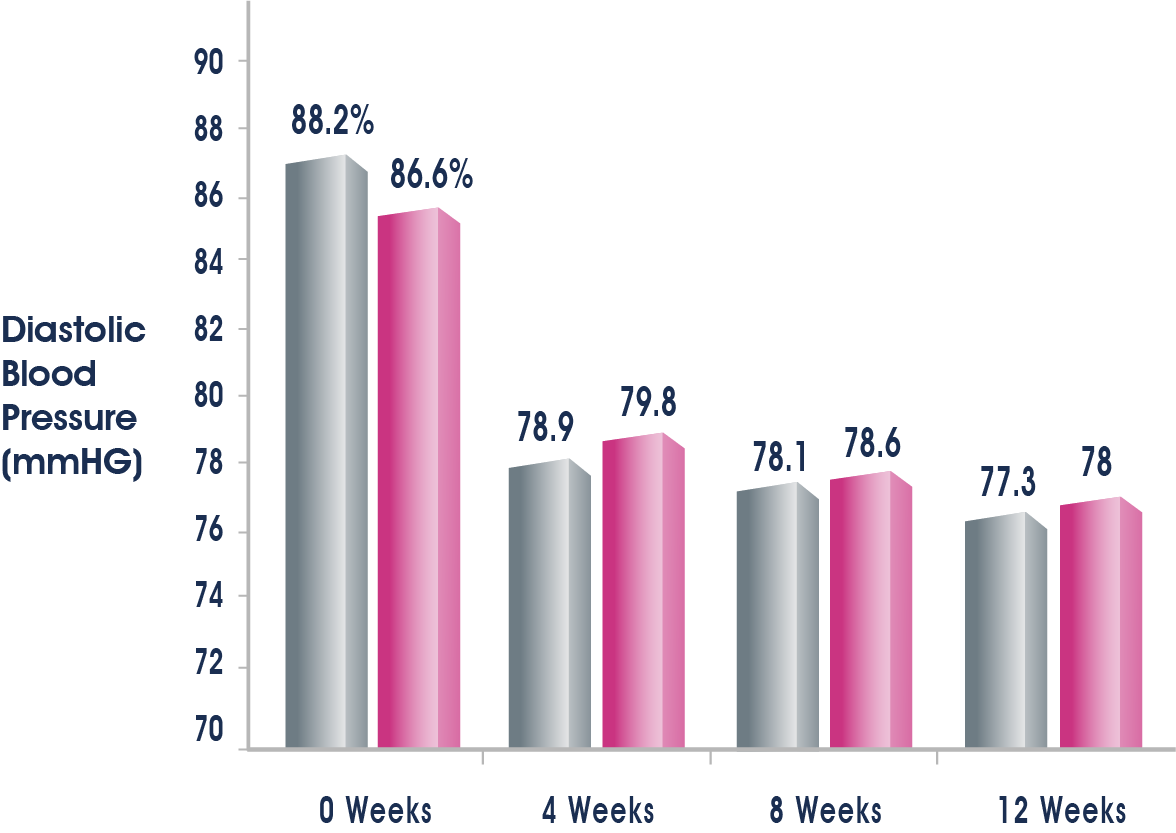

Significant decreases in office BP were observed from 4 weeks onward in the AML add-on group and the IRB add-on group, indicating a sustained antihypertensive effect for 12 weeks.5
BP: Blood Pressure; AML: Amlodipine; IRB: Irbesartan.
can get approximately 70% of patients achieve the target BP5
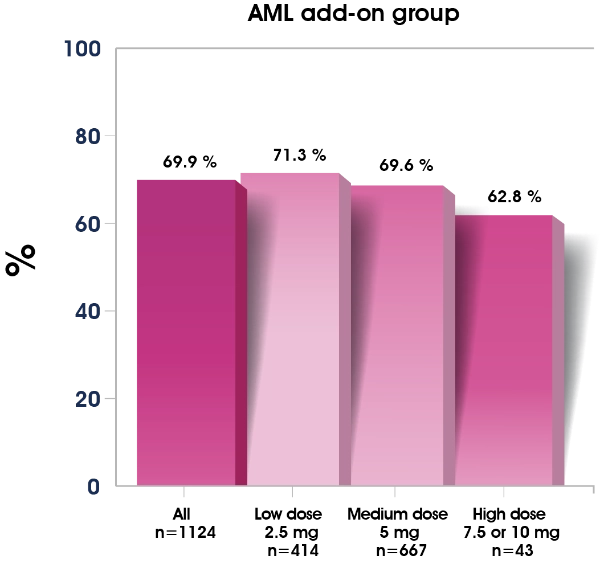
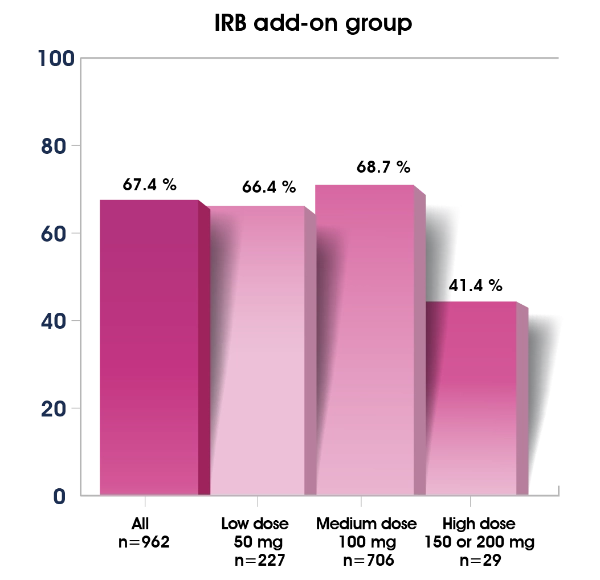
Two-thirds of hypertensive patients need a combination antihypertensive therapy to achieve the target blood pressure (BP).5
is superior to the combination of the Valsartan 80mg/day and Amlodipine 5 mg/day in decreasing BP7
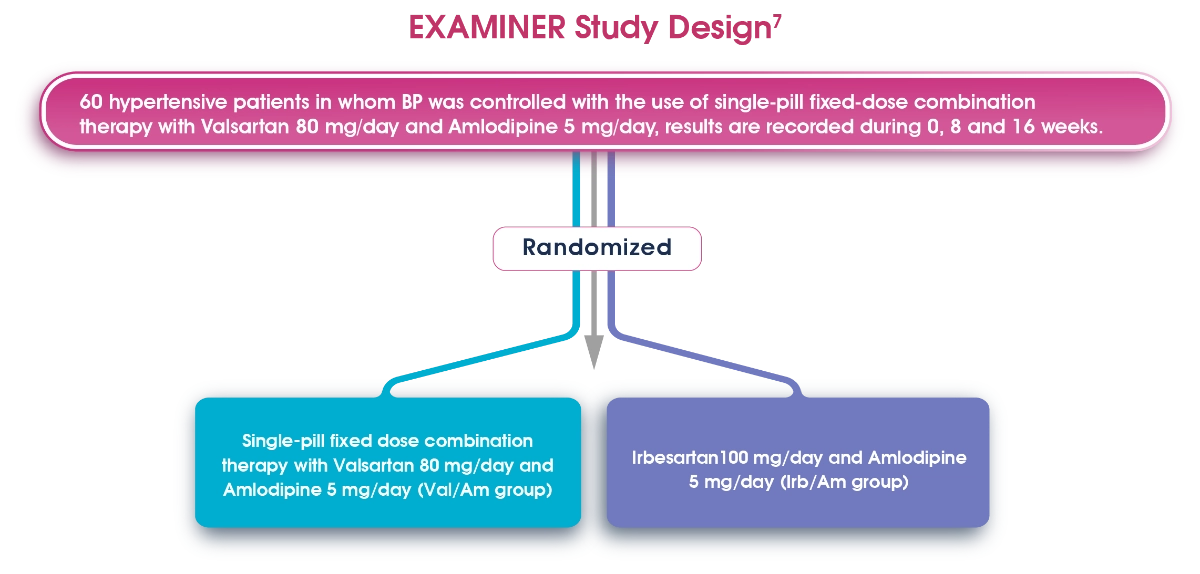
8 patients withdrew during the study:
-
1 patient in each group due to their admission to hospital with other diseases.
-
2 patients in the Irb/Am group, they didn’t visit the hospital and 1 in Val/Am group.
-
2 patients Irb/Am group due to study cancellation.
-
1 patient in the Val/Am group due to hypotension.
These two groups were extracted to examine the efficacy and safety of AML and IRB combination.
Finally analyzed 52 hypertensive patients:
- 24 patients in the Irb/Am group
- 28 patients in Val/Am group
Trial Objective: To examine the therapeutic advantage of combination of antihypertensive drug therapy using amlodipine and irbesartan in hypertensive patients.
Conclusion: The combination therapy with AML and IRB swiftly and certainly lowers BP with a small chance of causing adverse effects. In addition, this combination is advantageous in lowering serum uric acid and is suitable for protecting kidney in CKD patients. Tablet containing AML and IRB seems promising in maintaining high adherence and exhibiting the benefits of this combination therapy efficiently.
AML, Amlodipine; IRB, Irbesartan.
Changes in SBP and DBP in patients in the groups who reached the target BP at 8 weeks.7
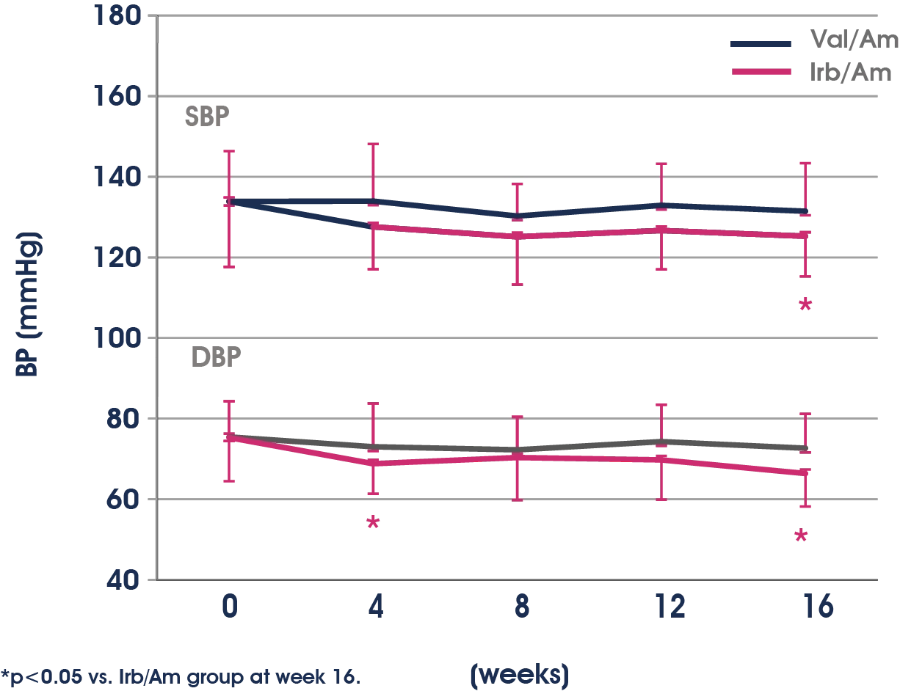
BP: Blood Pressure; AML: Amlodipine; IRB: Irbesartan; Val: Valsartan; SBP: Systolic blood pressure, DBP: Diastolic blood pressure.

significantly decreases serum UA & TG compared with combination therapy with Valsartan and Amlodipine.7
Changes in serum UA at 0, 8, 16 weeks in the Val/Am and Irb/Am subgroups.7
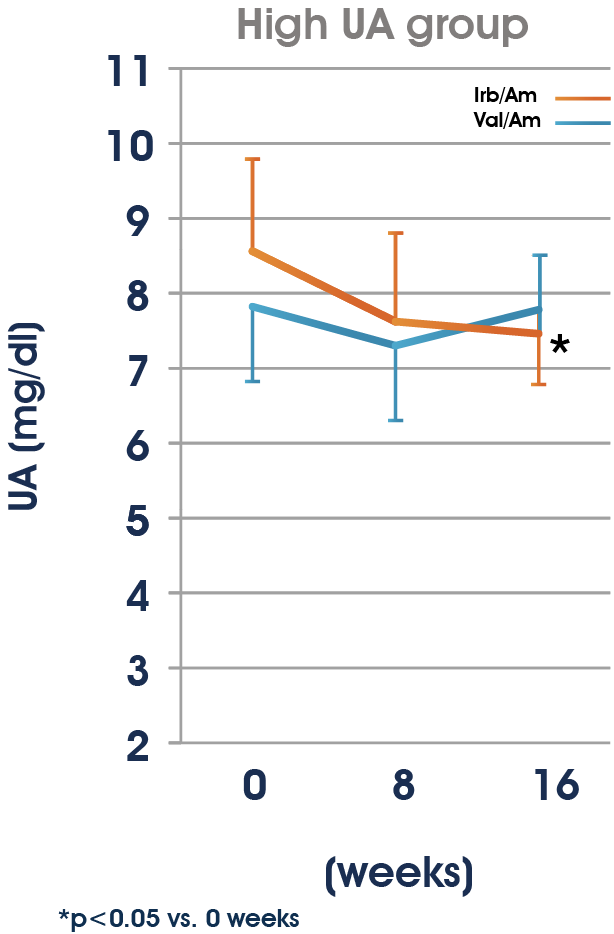
Changes in the lipid profile at 0, 8 and 16 weeks Val/Am and Irb/Am groups.7
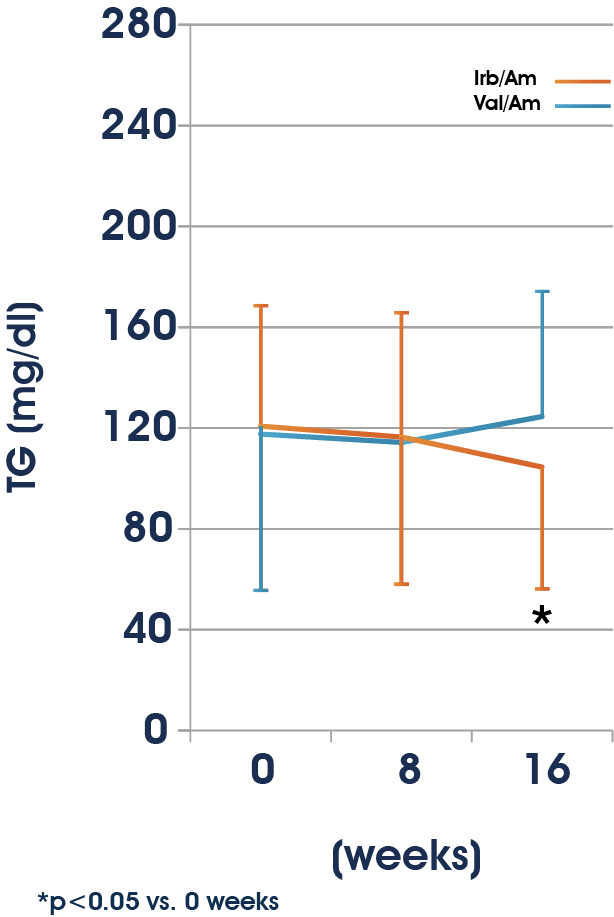
BP: Blood Pressure; AML: Amlodipine; IRB: Irbesartan; Val: Valsartan; SBP: Systolic blood pressure, DBP: Diastolic blood pressure, UA: Uric Acid, TG: Triglycrides.
Why adding an ARB to a CCB may reduce the incidence of oedema8,9
- Calcium channel blockers (CCBs) can cause arterial dilatation8
- This increases the intracapillary pressure, exuding fluid into the interstitium9
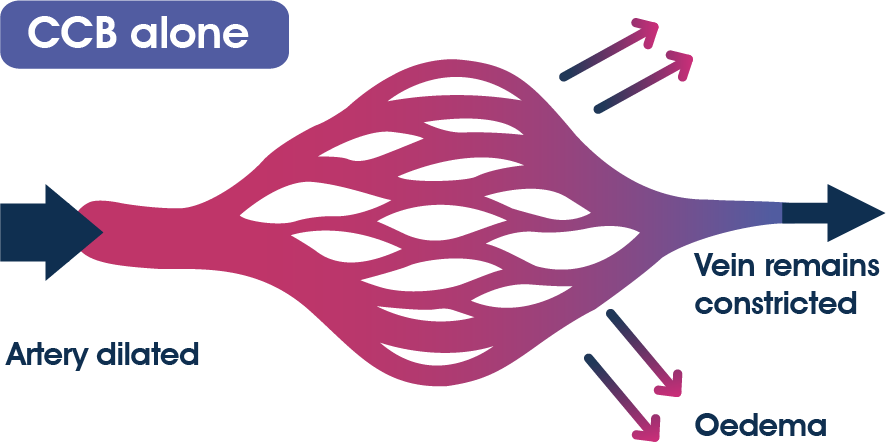
- Adding an angiotensin II receptor blocker (ARB) to a CCB reduces the incidence of oedema9
- Adding an ARB the arterial pressure also further lowers9
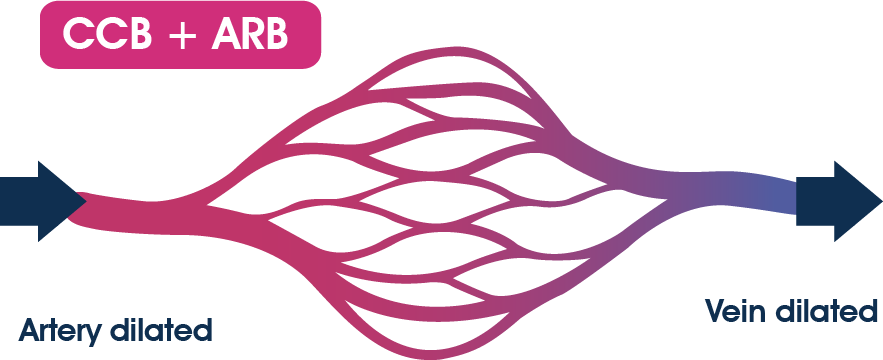
The combination of an ARB with CCB lowers the incidence of peripheral oedema when compared to CCB monotherapy.8
In a meta-analysis of 7 studies with 3,909 patients, the combination of an ARB and amlodipine had a significantly lower risk of adverse events than amlodipine monotherapy10
Pooled incidence of peripheral oedema and withdrawal due to oedema with CCB monotherapy and CCB/RAS blocker combination8
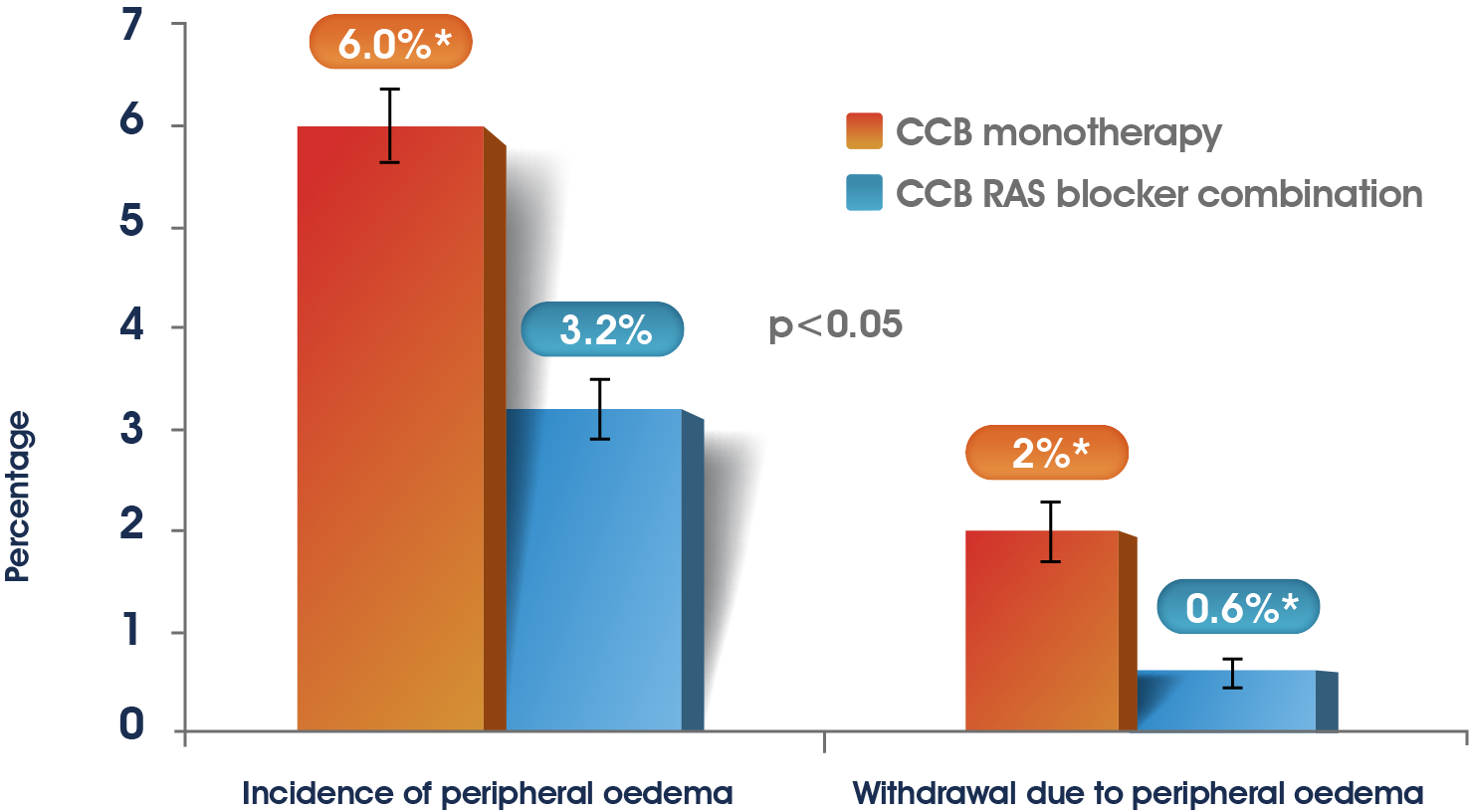
Systematic review of 25 randomized controlled trials with 17,206 patients reporting the incidence
of peripheral oedema or withdrawal of patients because of oedema and a total sample size more than 1008
The combination of an ARB with Amlodipine is generally well tolerated10
CCB: calcium channel blocker; RAS: renin-angiotensin system; ARB: Angiotensin Receptor blocker.
- Aprovasc. Summary of Product Characteristics. Saudi Arabia. 2015.
- DiPette DJ, et al. Fixed-dose combination pharmacologic therapy to improve hypertension control worldwide: Clinical perspective and policy implications. J Clin Hypertens. 2019; 21 (1): 4-15.
- Bobrie G. I-COMBINE study: assessment of efficacy and safety profile of irbesartan/amlodipine fixeddose combination therapy compared with amlodipine monotherapy in hypertensive patients uncontrolled with amlodipine 5 mg monotherapy: a multicenter, phase III, prospective, randomized, open-label with blinded-end point evaluation study. Clin Ther. 2012; 34 (8):1705-19.
- Bobrie G. I-ADD study: assessment of efficacy and safety profile of irbesartan/amlodipine fixed-dose combination therapy compared with irbesartan monotherapy in hypertensive patients uncontrolled with irbesartan 150 mg monotherapy: a multicenterphase III, prospective, randomized, open-label with blinded-end point evaluation study. Clin Ther. 2012; 34 (8): 1720-34 e3.
- Ishimitsu T, et al. The therapeutic advantage of combination antihypertensive drug therapy using amlodipine and irbesartan in hypertensive patients: Analysis of the post-marketing survey data from PARTNER (Practical combination therapy of Amlodin and angiotensin II Receptor blocker; safety and efficacy in patients with hypertension) study. Clin Exp Hypertens. 2015; 37 (7): 542-50.
- Sica DA. Rationale for fixed-dose combinations in the treatment of hypertension: the cycle repeats. Drugs. 2002; 62 (3): 443-62.
- Motozato K, Miura S, Shiga Y, et al. Efficacy and safety of two single-pill fixed-dose combinations of angiotensin II receptor blockers/calcium channel blockers in hypertensive patients (EXAMINER study). Clin Exp Hypertens. 2016;38(1):45–50.
- Makani H, et al. Effect of renin-angiotensin system blockade on calcium channel blocker-associated peripheral edema. Am J Med. 2011; 124 (2): 128-35.
- Messerli FH. Vasodilatory edema: a common side effect of antihypertensive therapy. Curr Cardiol Rep. 2002; 4 (6): 479-82.
- Ma J, et al. Meta-analysis of the efficacy and safety of adding an angiotensin receptor blocker (ARB) to a calcium channel blocker (CCB) following ineffective CCB monotherapy. J Thorac Dis. 2015; 7 (12): 2243-52.
MAT-SA-2200364/V1/April 2022