ACC/AHA vs ESC/EAS LDL–C recommendations for residual risk reduction in ASCVD: A simulation study from Da Vinci

Key Takeaway
This simulation study from Da Vinci identified notable differences between the 2019 ESC/EAS and 2018 ACC/AHA guidelines in their clinical approach to LLT in patients with ASCVD. The study also identified that:
- About 80–85% of the patients* were on monotherapy based LLT
- Patients achieving 2018 ACC/AHA (<70 mg/dL) vs 2019 ESC/EAS (<55 mg/dL) goals were 39% vs 19%
- Achievement of LDL−C <70 mg/dL was more likely in patients receiving combination therapy with either ezetimibe or a PCSK9i vs patients on statin monotherapy
- In patients with LDL−C ≥70 mg/dL, to achieve LDL−C levels of <70 mg/dL, <55 mg/dL and <40 mg/dL, median LDL−C reductions of 26%, 42% and 58% would be needed, respectively
- In patients with LDL–C ≥70 mg/dL vs <70 mg/dL, the estimated 10–year risk of CV events were 32% vs 35%
- Attaining 2018 ACC/AHA or 2019 ESC/EAS goals resulted in simulated ARRs of 4% and 6%, respectively
- For implementation of the guidelines, greater use of combination therapies would be required
- The residual risk among patients with ASCVD receiving statins could be mitigated if 2019 ESC/EAS recommendations were achieved‡
- More stringent 2019 ESC/EAS goals are expected to give better health outcomes vs 2018 ACC/AHA approach
Why This Matters
- LDL–C recommendations differ between the 2018 ACC/AHA approach and 2019 ESC/EAS guidelines for patients with ASCVD.
- The 2018 ACC/AHA guidelines recommend targeted reduction LDL–C <70 mg/dL§, in patients at very–high risk.
- The 2019 ESC/EAS guidelines recommend a stricter LDL–C goal of <55 mg/dL.
- Using DA VINCI study cohort, the extent of risk that could be mitigated by adopting 2018 ACC/AHA vs 2019 ESC/EAS LDL−C recommended approaches was simulated.
Study Design
This is a simulation study from Da Vinci. The methods and primary outcomes of Da Vinci study can be obtained from the link: Da Vinci.
- LLT use across the populations
- LDL–C control in patients with established ASCVD and stratified by ASCVD type¶
- Patients with LDL–C >70 mg/dL vs achievement of LDL–C <55 mg/dL
- Patients achieving LDL–C <40 mg/dL
- Implications of current practice and LDL–C goal achievement in future CV risk
Key Results
Overall, 2,039 patients with ASCVD (23% with CAD; 37% with CBD and 40% with PAD) were on stabilized LLT at the time of LDL–C measurement.
LLT Use in patients with ASCVD
| Type of LLT | Patients using LLT (%) |
|
Statin monotherapy |
Used most frequently |
| Moderate–intensity statins# as monotherapy | Ranged from 40.4% among patients with CAD to 48.7% in patients with CBD |
| High–intensity statins# | CAD: 51.1%; CBD: 39.7%; PAD: 39.1% |
| Ezetimibe in combination with statins|| | CAD: 15.3%; CBD: 6.7%; PAD: 8.2% |
| PCSK9i in combination with statins and/or ezetimibe|| | CAD: 0.4%; CBD: 1.2%; PAD: 1.6% |
Proportion of patients achieving LDL–C Levels
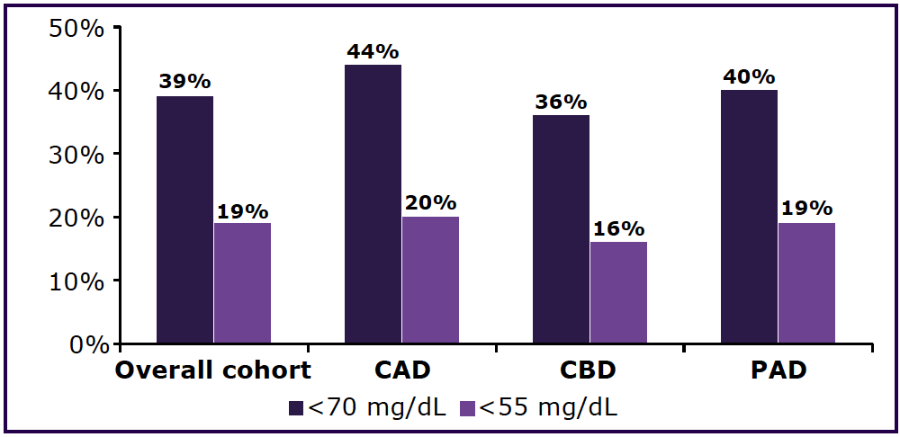
- Achievement of an LDL–C level <70 mg/dL was more likely in patients receiving combination therapy with either ezetimibe or a PCSK9i vs patients on statin monotherapy.
- Despite of using PSCK9i infrequently, 58% of patients receiving PSCK9i in combination with other LLT have attained LDL–C level of <55 mg/dL.
Residual risk among the patients
| LDL–C Levels | Patients (%) | Median (IQR) LDL–C Level | Median (IQR) Predicted 10–year CV risk |
| ≥70 mg/dL | 61% | 93 (81–115) mg/dL | 32% (25–43%) |
| <70 mg/dL** | 39% | 56 (46–63) mg/dL | 35% (26–46%) |
Simulated risk reduction in patients with established ASCVD (LDL–C Level of ≥70 mg/dL)
| LDL–C Levels | Median 10–year CV risk | Median RRR of CV events | Median ARR of CV events |
Required median
|
AR to lower LDL–C levels to 69 mg/dL |
| <70 mg/dL | 28% | 14% | 4% | 26% | 24 mg/dL (12–46) |
| <55 mg/dL | 25% | 22% | 6% | 42% | 39 mg/dL (27–91) |
| <40 mg/dL | 23% | 29% | 8% | 58% | 54 mg/dL (42–76) |
For additional information about simulated risk reduction, please click on the hyperlink.
Limitations
- Over 90% of patients were white (homogenous ethnicity).
- Simulation might have underestimated CV risk and ARR in very high-risk patients.
- Use of LLT may vary across countries and might not necessarily reflect practice in other regions.
- The study sites might have focused on lipid management and prevention of CV events. Hence, the study findings are likely to present better than average management scenario.
For additional details, please refer the source publication Vallejo-Vaz AJ, et al.
* Most of the patients with major manifestations of ASCVD
† Probably due to additional comorbidities like diabetes, history of smoking and increased use of more potent LLTs including combination therapies.
‡ In a population like Da Vinci cohort § Using 70 mg/dL as a limit to guide additional LLT
¶ As per 2019 ESC/EAS guidelines, all patients are at very–high risk
# With or without other LLT || High/moderate/unknown intensity
** Had slightly higher prevalence of risk factors such as a history of smoking and diabetes (50.7%)
ARR, absolute risk reduction; ACC/AHA, American College of Cardiology/ American Heart Association; ASCVD, atherosclerotic cardiovascular disease; CAD, coronary artery disease; CBD, cerebrovascular disease; CV, cardiovascular; ESC/EAS, European Society of Cardiology/European Atherosclerosis Society; IQR, interquartile range; LDL–C, low–density lipoprotein cholesterol; LLT, lipid lowering therapy; PSCK9i, proprotein convertase subtilisin/kexin type 9 inhibitors; PAD, peripheral artery disease; RR, risk reduction; RRR, relative risk reduction.
- Vallejo-Vaz AJ, Bray S, Villa G, Brandts J, Kiru G, Murphy J, et al. Implications of ACC/AHA versus ESC/EAS LDL–C recommendations for residual risk reduction in ASCVD: A simulation study from DA VINCI. Cardiovasc Drugs Ther. 2022. doi: 10.1007/s10557-022-07343-x. Epub ahead of print. PMID: 35567726.