A deeper look at the inflammation behind exacerbations can IGNITE NEW THINKING IN COPD

Each Copd Exacerbation May Increase the Risk of Another, Putting Patients’ Lives at Greater Risk
Exacerbation risk accelerates after each exacerbation1
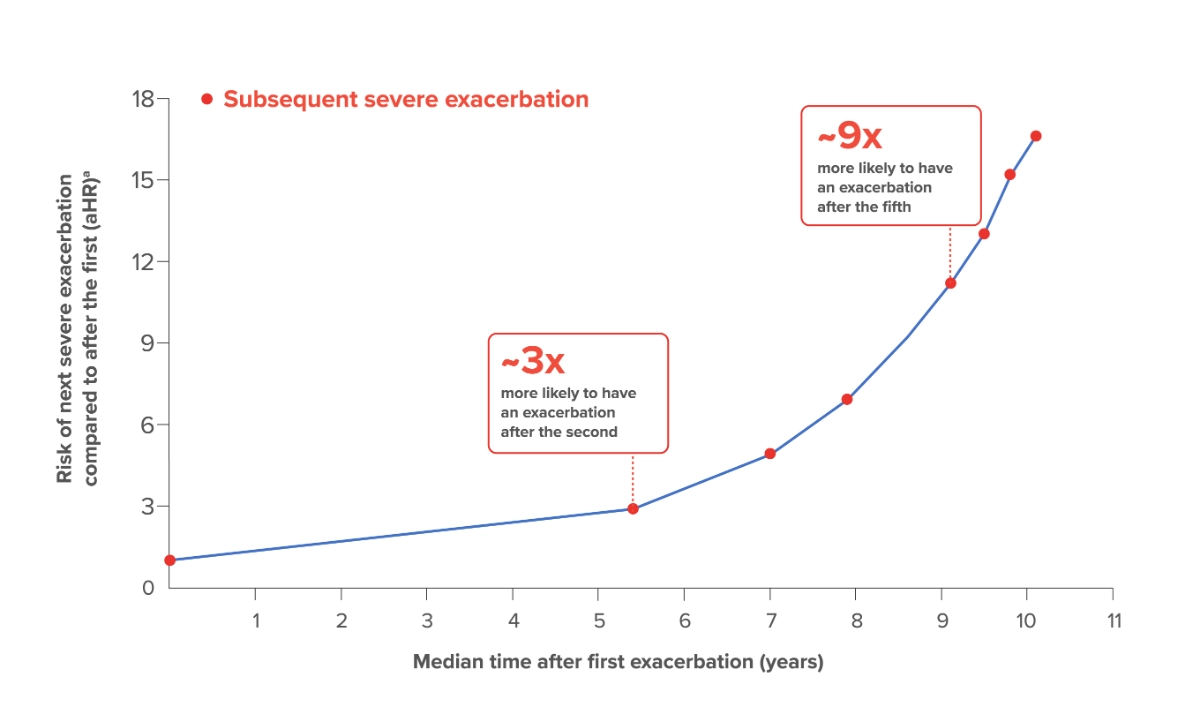
Based on data from a large population-based cohort of 73,106 Canadian patients who were hospitalized for the first time because of a severe exacerbation of COPD (1990-2005, followed until death or March 31, 2007) with a median follow-up of 3.6 years (range 1 day to 17 years). The mean age of patients in this retrospective study was 75 years old.1
aAdjusted for age, sex, calendar time, and the modified Chronic Disease Score.1
Exacerbations have been shown to accelerate lung function decline2
Significant lung function decline may occur even after a single COPD exacerbation2
- The annual decline in postbronchodilator FEV1 nearly doubled after 1 moderate-to-severe exacerbation (pre-exacerbation 39.1 mL/year vs 76.5 mL/year postexacerbation [P=0.003])2,b
bBased on data from a retrospective analysis of 586 patients with moderate-to-severe (postbronchodilator FEV1 70% of the predicted normal and FEV1 70% of FVC) COPD participating in the 4-year, randomized, double-blind, placebo-controlled, parallel-group UPLIFT trial.
Exacerbations may increase morbidity risk3-6
Patients with exacerbations leading to hospitalization are at an increased risk for hospital readmissions
- Up to 35% of patients were readmitted within 90 days following an exacerbation3-5,c
COPD exacerbations are associated with a worsening of symptoms that can seriously impact quality of life
Patients typically experience:

Limited activity levels and
exercise capacity6

Fatigue7

Sleep-related disturbances8,9

Anxiety and depression8
cBased on data from an investigation that examined outcomes (in-hospital and 90-day postdischarge mortality and 90-day readmission) in patients with a severe COPD exacerbation (n=15,191) seen within the European COPD Audit.3
Exacerbations may increase mortality risk1
After second exacerbationd

~2x
higher riske
After fifth exacerbationd
~3x
higher riske
Noteworthy
All-cause mortality data showf: 50% of patients died less than 4 years after their first COPD-related hospitalization1,d
dBased on data from a large population-based cohort of 73,106 Canadian patients who were hospitalized for the first time because of a severe exacerbation of COPD (1990-2005, followed until death or March 31, 2007) with a median follow-up of 3.6 years (range 1 day to 17 years). The mean age of patients in this retrospective study was 75 years old.
eRelative risk of mortality compared to the first exacerbation (adjusted hazard ratio).
fThe median survival was 3.6 years.
Chronic Underlying Inflammation Drives the Downward Spiral of Copd Progression10-18
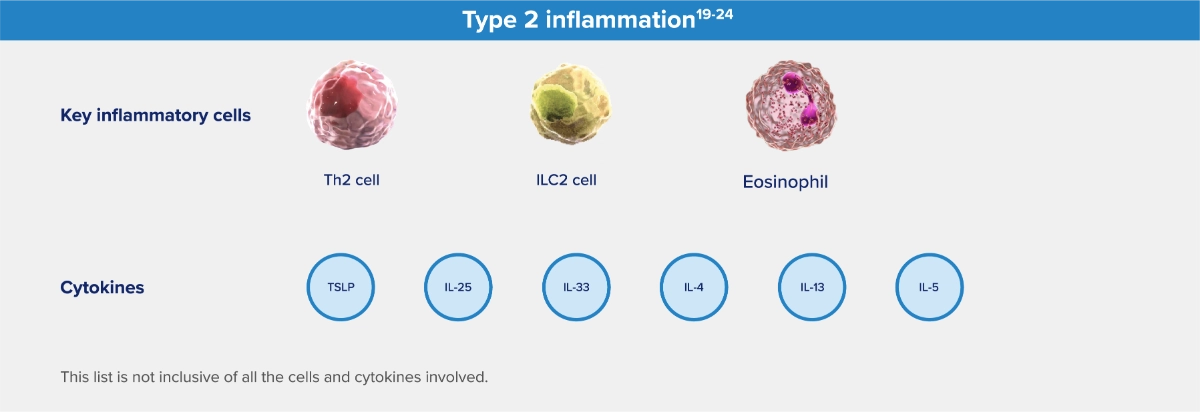
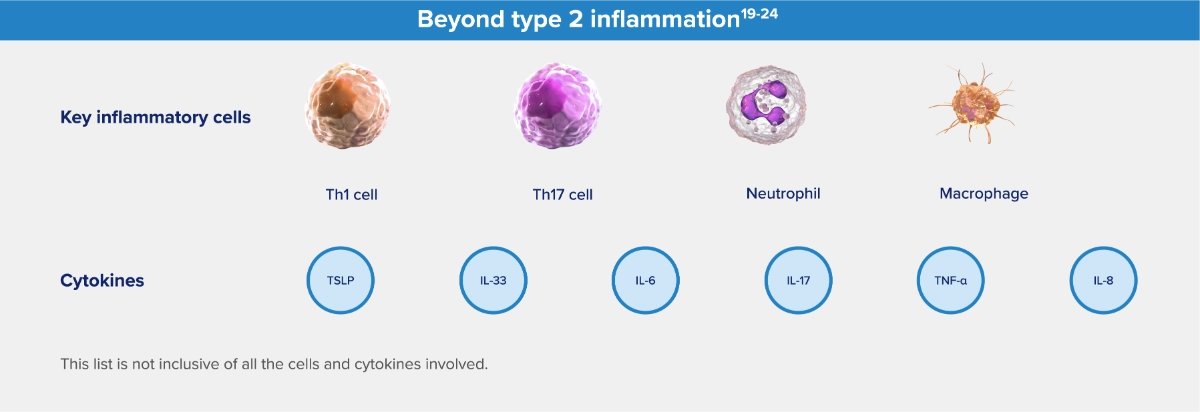
Different types of chronic inflammation have an important role in COPD pathophysiology
Many cell types and cytokines are involved in these processes, including:
Noteworthy
Up to 37% of COPD patients without an asthma comorbidity had evidence of type 2 inflammation25-29,g
gBased on findings from 5 studies in COPD patients without asthma. Eosinophil levels used to define type 2 inflammation ranged from ≥300 cells/μL to ≥340 cells/μL (blood), ≥2% (blood and sputum), or >3% nonsquamous cells (sputum). Percentages of patients with type 2 inflammation ranged from 12.3% to 37%.25-29
Type 2 inflammation may drive poor outcomes in COPD9,30,31
Type 2 inflammation encompasses both type 2 effector cells (eg, Th2, ILC2, eosinophils, and mast cells) and key cytokines
(eg, IL-4, IL-13, and IL-5)16,19,20,32-41
Airflow Obstruction

Persistent symptoms (dyspnea,
chronic cough, sputum)9
Progressive lung function decline9

Exacerbations9
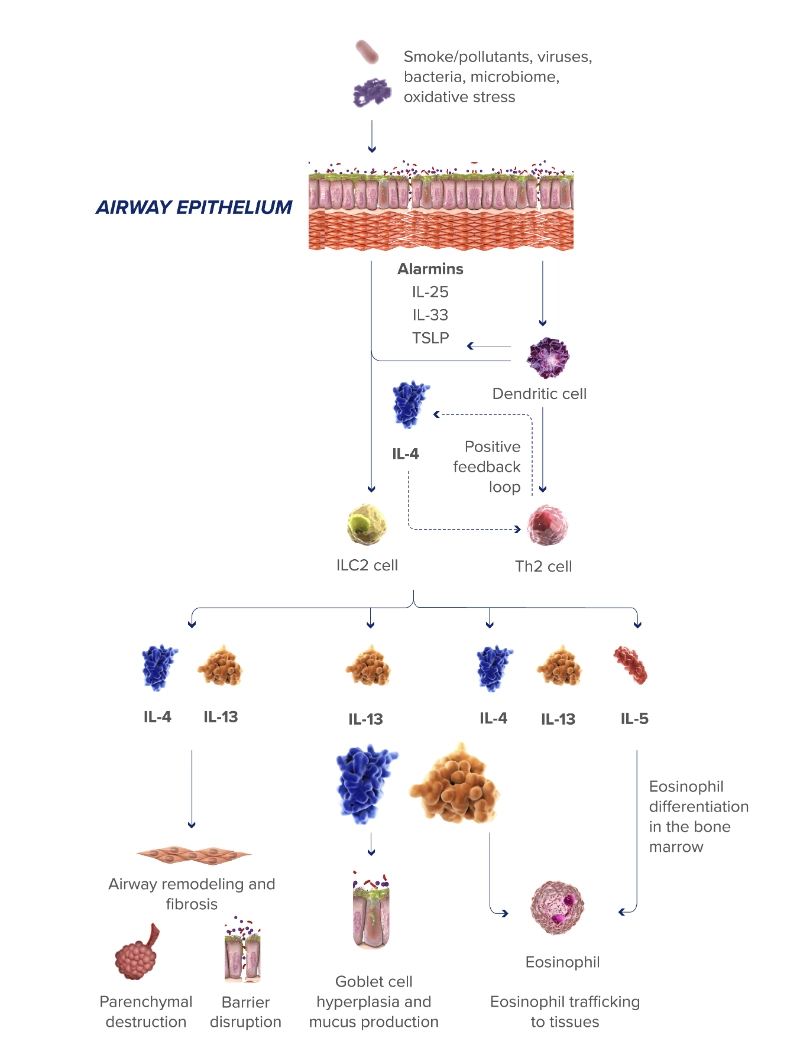
Select cytokines play important roles in type 2 inflammation
IL-4 and IL-13 drive inflammatory cell activity
IL-4 and IL-13 promote the activation and trafficking of type 2 inflammatory cells, including eosinophils, to the lungs, which may contribute to airway remodeling and parenchymal destruction in COPD32,34,42-48
The critical role of IL-13 in airflow limitation
IL-13 plays a role in emphysema, fibrosis, and goblet cell hyperplasia and increases expression of MUC5AC, a major constituent of airway mucus17,33,34,48-51
The role of IL-33
IL-33 initiates and amplifies the broad inflammatory cascades in COPD, inclusive of type 2 inflammation and beyond22,23
The role of IL-5
IL-5 is required for the growth and differentiation, recruitment, activation, and survival of eosinophils, which may be biomarkers of a broader type 2 inflammatory response32
Look for Elevated Blood Eosinophils (≥300 Cells/μl)—a Biomarker of Type 2 Inflammation in Copd9,31
Identifying COPD patients with type 2 inflammation may help determine those at increased risk of exacerbations
Blood eosinophils
≥300
cells/μL

32%
increased risk of
COPD exacerbations30,h,i
hResults from an observational analysis of 1553 patients with GOLD spirometry grade 2-4 COPD evaluating the relationship between blood eosinophil counts and COPD exacerbation risk.30
iStratified analysis confirmed that increased exacerbation risk was driven by subjects with a history of frequent exacerbations, defined as ≥2 exacerbations per year.
Elevated eosinophils and a history of frequent exacerbations help identify patients and guide treatment options9,52
According to GOLD 2023 recommendations, patients with frequent exacerbations (GOLD Group E) and blood eosinophils ≥300 cells/μL may receive an ICS in combination with LABA + LAMA9
Noteworthy
Even when treatment is optimized with inhaled triple therapy, many patients with COPD may continue to experience exacerbations52
Understanding type 2 inflammation in COPD may help shed light on why some patients continue to experience exacerbations
aHR, adjusted hazard ratio; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; ILC2, type 2 innate lymphoid cell; LABA, long-acting beta agonist; LAMA, long-acting muscarinic antagonist; MUC5AC, mucin 5AC; TNF, tumor necrosis factor; TSLP, thymic stromal lymphopoietin.
- Suissa S, Dell’Anello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957-963.
- Halpin DMG, Decramer M, Celli BR, Mueller A, Metzdorf N, Tashkin DP. Effect of a single exacerbation on decline in lung function in COPD. Respir Med. 2017;128:85-91.
- Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, et al. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD Audit. Eur Respir J. 2016;47(1):113-121.
- Shah T, Churpek MM, Peraillon MC, Konetzka RT. Understanding why patients with COPD get readmitted. A large national study to delineate the Medicare population for the readmissions penalty expansion. Chest. 2015;147(5):1219-1226.
- Press VG, Myers LC, Feemster LC. Preventing COPD readmissions under the Hospital Readmissions Reduction Program. How far have we come? Chest. 2021;159(3):996-1006.
- Jones SE, Barker RE, Nolan CM, Patel S, Maddocks M, Man WDC. Pulmonary rehabilitation in patients with an acute exacerbation of chronic obstructive pulmonary disease. J Thorac Dis. 2018;10(suppl 12):S1390-S1399.
- Goërtz YMJ, Spruit MA, Van’t Hul AJ, et al. Fatigue is highly prevalent in patients with COPD and correlates poorly with the degree of airflow limitation. Ther Adv Respir Dis. 2019;13:1753466619878128. doi:10.1177/1753466619878128
- Miravitlles M, Worth H, Soler Cataluña JJ, et al. Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: results from the ASSESS study. Respir Res. 2014;15(1):122. doi:10.1186/s12931-014-0122-1
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 report). Accessed [April 27, 2023]. https:// goldcopd.org/2023-gold-report-2/
- Cosio Piqueras MG, Cosio MG. Disease of the airways in chronic obstructive pulmonary disease. Eur Respir J. 2001;18(suppl 34):41s-49s.
- Tajti G, Gesztelyi R, Pak K, et al. Positive correlation of airway resistance and serum asymmetric dimethylarginine level in COPD patients with systemic markers of low-grade inflammation. Int J Chron Obstruct Pulmon Dis. 2017;12:873-884.
- Higham A, Quinn AM, Cançado JED, Singh D. The pathology of small airways disease in COPD: historical aspects and future directions. Respir Res. 2019;20(1):49. doi:10.1186/s12931-019-1017-y
- O’Donnell DE, Parker CM. COPD exacerbations. 3: Pathophysiology. Thorax. 2006;61(4):354-361.
- Calverley PMA. Respiratory failure in chronic obstructive pulmonary disease. Eur Respir J. 2003;22(suppl 47):26s-30s.
- Roussos C, Koutsoukou A. Respiratory failure. Eur Respir J. 2003;22(suppl 47):3s-14s.
- Aghapour M, Raee P, Moghaddam SJ, Hiemstra PS, Heijink IH. Airway epithelial barrier dysfunction in chronic obstructive pulmonary disease: role of cigarette smoke exposure. Am J Respir Cell Mol Biol. 2018;58(2):157-169.
- Brightling CE, Saha S, Hollins F. Interleukin-13: prospects for new treatment. Clin Exp Allergy. 2010;40(1):42-49.
- Barberà JA, Peinado VI, Santos S. Pulmonary hypertension in chronic obstructive pulmonary disease. Eur Respir J. 2003;21(5):892-905.
- Oishi K, Matsunaga K, Shirai T, Hirai K, Gon Y. Role of type 2 inflammatory biomarkers in chronic obstructive pulmonary disease. J Clin Med. 2020;9(8):2670. doi:10.3390/ jcm9082670
- Yousuf A, Ibrahim W, Greening NJ, Brightling CE. T2 biologics for chronic obstructive pulmonary disease. J Allergy Clin Immunol Pract. 2019;7(5):1406-1416.
- Barnes PJ. Inflammatory endotypes in COPD. Allergy. 2019;74(7):1249-1256.
- Gabryelska A, Kuna P, Antczak A, Białasiewicz P, Panek M. IL-33 mediated inflammation in chronic respiratory diseases—understanding the role of the member of IL-1 superfamily. Front Immunol. 2019;10:692. doi:10.3389/ fimmu.2019.00692
- Allinne J, Scott G, Lim WK, et al. IL-33 blockade affects mediators of persistence and exacerbation in a model of chronic airway inflammation. J Allergy Clin Immunol. 2019;144(6):1624-1637.e10.
- Calderon AA, Dimond C, Choy DF, et al. Targeting interleukin-33 and thymic stromal lymphopoietin pathways for novel pulmonary therapeutics in asthma and COPD. Eur Respir Rev. 2023;32(167):220144. doi:10.1183/16000617.0144-2022
- Oshagbemi OA, Franssen FME, van Kraaij S, et al. Blood eosinophil counts, withdrawal of inhaled corticosteroids and risk of COPD exacerbations and mortality in the clinical practice research datalink (CPRD). COPD. 2019;16(2):152-159.
- Casanova C, Celli BR, de-Torres JP, et al. Prevalence of persistent blood eosinophilia: relation to outcomes in patients with COPD. Eur Respir J. 2017;50:1701162. doi:10.1183/13993003.01162-2017
- Singh D, Kolsum U, Brightling CE, Locantore N, Agusti A, Tal-Singer R; on behalf of the ECLIPSE investigators. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44(6):1697-1700.
- Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662-671.
- Oshagbemi OA, Burden AM, Braeken DCW, et al. Stability of blood eosinophils in patients with chronic obstructive pulmonary disease and in control subjects, and the impact of sex, age, smoking, and baseline counts. Am J Respir Crit Care Med. 2017;195(10):1402-1404.
- Yun JH, Lamb A, Chase R, et al; for the COPDGene and ECLIPSE Investigators. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141(6):2037-2047.e10.
- Bélanger M, Couillard S, Courteau J, et al. Eosinophil counts in first COPD hospitalizations: a comparison of health service utilization. Int J Chron Obstruct Pulmon Dis. 2018;13:3045-3054.
- Gandhi NA, Bennett BL, Graham NMH, Pirozzi G, Stahl N, Yancopoulos D. Targeting proximal drivers of type 2 inflammation in disease. Nat Rev Drug Discov. 2016;15(1):35-50.
- Alevy YG, Patel AC, Romero AG, et al. IL-13–induced airway mucus production is attenuated by MAPK13 inhibition. J Clin Invest. 2012;122(12):4555-4568.
- Doyle AD, Mukherjee M, LeSuer WE, et al. Eosinophil-derived IL-13 promotes emphysema. Eur Respir J. 2019;53(5):1801291. doi:10.1183/13993003.01291-2018
- Cooper PR, Poll CT, Barnes PJ, Sturton RG. Involvement of IL-13 in tobacco smoke-induced changes in the structure and function of rate intrapulmonary airways. Am J Respir Cell Mol Biol. 2010;43(2):220-226.
- Arora S, Dev K, Agarwal B, Das P, Syed MA. Macrophages: their role, activation, and polarization in pulmonary diseases. Immunobiology. 2018;223(4-5):383-396.
- He S, Xie L, Lu J, Sun S. Characteristics and potential role of M2 macrophages in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:3029-3039.
- Wang Z, Bafadhel M, Haldar K, et al. Lung microbiome dynamics in COPD exacerbations. Eur Respir J. 2016;47(4):1082-1092.
- Linden D, Guo-Parke H, Coyle PV, et al. Respiratory viral infection: a potential “missing link” in the pathogenesis of COPD. Eur Respir Rev. 2019;28(151):180063. doi:10.1183/16000617.0063-2018
- Wang X, Xu C, Ji J, et al. IL-4/IL-13 upregulates Sonic hedgehog expression to induce allergic airway epithelial remodeling. Am J Physiol Lung Cell Mol Physiol. 2020;318(5):L888-L899.
- Saatian B, Rezaee F, Desando S, et al. Interleukin-4 and interleukin-13 cause barrier dysfunction in human epithelial cells. Tissue Barriers. 2013;1(2):e24333. doi:10.4161/tisb.24333
- Rosenberg HF, Phipps S, Foster PS. Eosinophil trafficking in allergy and asthma. J Allergy Clin Immunol. 2007;119(6):1303-1310.
- Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16-27.
- Defrance T, Carayon P, Billian G, et al. Interleukin 13 is a B cell stimulating factor. J Exp Med. 1994;179(1):135-143.
- Yanagihara Y, Ikizawa K, Kajiwara K, Koshio T, Basaki Y, Akiyama K. Functional significance of IL-4 receptor on B cells in IL-4–induced human IgE production. J Allergy Clin Immunol. 1995;96(6 pt 2):1145-1151.
- Gandhi NA, Pirozzi G, Graham NMH. Commonality of the IL-4/IL-13 pathway in atopic diseases. Expert Rev Clin Immunol. 2017;13(5):425-437.
- Kaur D, Hollins F, Woodman L, et al. Mast cells express IL-13Rα1: IL-13 promotes human lung mast cell proliferation and FcεRI expression. Allergy. 2006;61(9):1047-1053.
- Zheng T, Zhu Z, Wang Z, et al. Inducible targeting of IL-13 to the adult lung causes matrix metalloproteinase– and cathepsin-dependent emphysema. J Clin Invest. 2000;106(9):1081-1093.
- Garudadri S, Woodruff PG. Targeting chronic obstructive pulmonary disease phenotypes, endotypes, and biomarkers. Ann Am Thorac Soc. 2018;15(suppl 4):S234-S238.
- Singanayagam A, Footitt J, Marczynski M, et al. Airway mucins promote immunopathology in virus-exacerbated chronic obstructive pulmonary disease. J Clin Invest. 2022;132(8):e12901. doi:10.1172/JCI120901
- Zhu Z, Homer RJ, Wang Z, et al. Pulmonary expression of interleukin-13 causes inflammation, mucus hypersecretion, subepithelial fibrosis, physiologic abnormalities, and eotaxin production. J Clin Invest. 1999;103(6):779-788.
- Halpin DMG, Dransfield MT, Han MK, et al. The effect of exacerbation history on outcomes in the IMPACT trial. Eur Respir J. 2020;55:1901921. doi:10.1183/13993003.01921-2019
